Based on data from the Bureau of Labor Statistics, the Department of Education, and independent studies, the Department of Health and Human Services (HHS) estimates a shortfall of approximately 51,000 qualified health IT workers over the next five years. To that end, on Friday, April 2, 2010, the (HHS) announced awards totaling $84 million to 16 universities and junior colleges to help support the training and development of more than 50,000 new health IT professionals. Read the link below
Educational Funding for 12 Key Healthcare IT Workforce Roles On the Way!
Saturday, December 4, 2010
Tuesday, November 30, 2010
Assessing the Value of IT: Understanding and Measuring the Link Between IT and Strategy
An organization is considering spending 18 months and millions of US dollars to implement a new business application. How does one know if this project will deliver any positive, quantifiable results to the organization? Exactly how are the costs of delivering these results and the value produced by the information technology going to be measured? Without a systematic approach toward the valuation of IT projects that includes a process for measuring progress toward specific, quantifiable business goals, most IT managers, cost accountants and auditors will not be able to answer these questions with confidence and justify the value of IT projects to the organization. This article defines a method for assessing the value of IT as it affects the strategic capabilities of the organization, vs. simple cost-efficiencies, by using the value chain to link IT projects to strategies and business processes
Assessing the Value of IT: Understanding and Measuring the Link Between IT and Strategy
Assessing the Value of IT: Understanding and Measuring the Link Between IT and Strategy
Monday, November 29, 2010
Home Health Services -mHealth
Organized home health in India is an untapped potential. Home health care is defined as rendering predominantly medically-related services to patients in a home setting rather than in a medical facility. Home health care may include skilled nursing in addition to speech, occupational and physical therapy. It also includes monitoring the patient's prescriptions. In an Indian context, assistance to activities of daily living does not seem to make much sense.
What are the challenges in putting together a home health delivery model?
-> Organizing a fleet of nurses and therapists (Logistics)
-> Maintaining longitudinal patient progress and history
-> Minimize manual documentation requirements
-> Lack of ability to compare the acquired data with reference values
-> Open source software to capture data at patient site
-> Sync up PC data to the Hospital Information System or EMR
-> Connectivity to the Internet at the patient premises for self monitoring
-> Medical device to PC or cellular connection using USB, wire or Bluetooth
-> Data transmission via broadband, GSM, CDMA to Hospital Information System
Some considerations:
(1) Use of wireless Body Area Networks (BAN) as an alternative to conventional monitor - Example: The disposable unit consists of a ECG patch, analog amplification circuit, battery, and radio transmitter that sends signals to a Wireless Handheld Device either through USB or Bluetooth. The handheld will connect to the Mobile Healthcare Platform of the Hospital Information System.
(2) Use of tele-health monitors that capture data from multiple devices and transmit data to back-end servers via broadband.
With advent of 3G networks and low cost broadband services and WiFi, connectivity to the back end servers will be easier than before.
(3) Evaluation of Free Open Source Software (FOSS) for mobile platform and its counterpart back end enterprise application is a challenge.
Based on survey conducted by Center for Social Research India for Novo Nordisk in 2006 for diabetes monitoring, Home based monitoring was 86% less than monitoring at hospital and 89% of the patients are self funded. For a sustainable model for the service provider, more number of people need to adopt home monitoring. Longitudinal information capture and automatic alerting, self reliance, logistical ease are good value proposals for patients to switch.
What are the challenges in putting together a home health delivery model?
-> Organizing a fleet of nurses and therapists (Logistics)
-> Maintaining longitudinal patient progress and history
-> Minimize manual documentation requirements
-> Lack of ability to compare the acquired data with reference values
-> Open source software to capture data at patient site
-> Sync up PC data to the Hospital Information System or EMR
-> Connectivity to the Internet at the patient premises for self monitoring
-> Medical device to PC or cellular connection using USB, wire or Bluetooth
-> Data transmission via broadband, GSM, CDMA to Hospital Information System
Some considerations:
(1) Use of wireless Body Area Networks (BAN) as an alternative to conventional monitor - Example: The disposable unit consists of a ECG patch, analog amplification circuit, battery, and radio transmitter that sends signals to a Wireless Handheld Device either through USB or Bluetooth. The handheld will connect to the Mobile Healthcare Platform of the Hospital Information System.
(2) Use of tele-health monitors that capture data from multiple devices and transmit data to back-end servers via broadband.
With advent of 3G networks and low cost broadband services and WiFi, connectivity to the back end servers will be easier than before.
(3) Evaluation of Free Open Source Software (FOSS) for mobile platform and its counterpart back end enterprise application is a challenge.
Based on survey conducted by Center for Social Research India for Novo Nordisk in 2006 for diabetes monitoring, Home based monitoring was 86% less than monitoring at hospital and 89% of the patients are self funded. For a sustainable model for the service provider, more number of people need to adopt home monitoring. Longitudinal information capture and automatic alerting, self reliance, logistical ease are good value proposals for patients to switch.
Concept to Reality – Home Health Services
A preamble to introducing a new service or product is the associated marketing plan also known as the business development plan. Successfully introducing organized home health in the market involves painstaking research to understand the segment that will be receptive to the offer, the target population that will consume the service, and the positioning of the service. The positioning must consider internal imperatives and external competitive forces and cover strategic and tactical dimensions. This note presents initial thoughts and consideration to drive the first steps of the initiative.
Some critical questions that the plan should address are as follows:
• Definition of home health
• Demographic analysis of the market
• Manpower requirements and logistics
• Competitive climate
• Use of technology in health monitoring
• Financial analysis and breakeven
• Infrastructure requirements
• Roadmap and milestones
• Key differentiators (business model)
• Early internal alignment
Few challenges:
• Most reports on Indian Hospital sector are expensive
• The requirements vary dramatically from urban to rural and among age groups
• No canned reports on home health
• Need to understand regulatory and liability constraints
• Need to work with technology vendors to demonstrate a workable prototype as a part of the study
A suggested approach to convert the concept to a tangible plan is to put together a funded task force. The funded team should consist of two sets of individuals. One group will work with the internal verticals to assess the viability of services offered under the proposed umbrella. The other team should focus on the market dynamics culling primary and secondary market intelligence data. The team should be very familiar with the corporate vision, operational expectations, and financials.
Some critical questions that the plan should address are as follows:
• Definition of home health
• Demographic analysis of the market
• Manpower requirements and logistics
• Competitive climate
• Use of technology in health monitoring
• Financial analysis and breakeven
• Infrastructure requirements
• Roadmap and milestones
• Key differentiators (business model)
• Early internal alignment
Few challenges:
• Most reports on Indian Hospital sector are expensive
• The requirements vary dramatically from urban to rural and among age groups
• No canned reports on home health
• Need to understand regulatory and liability constraints
• Need to work with technology vendors to demonstrate a workable prototype as a part of the study
A suggested approach to convert the concept to a tangible plan is to put together a funded task force. The funded team should consist of two sets of individuals. One group will work with the internal verticals to assess the viability of services offered under the proposed umbrella. The other team should focus on the market dynamics culling primary and secondary market intelligence data. The team should be very familiar with the corporate vision, operational expectations, and financials.
Weaving IT into Organizational Strategy
Information technology has progressively moved from the periphery to the center of corporate strategy. This brief is not a prescription or an exhaustive recommendation but only brings to fore some of points to trigger in depth analysis on IT-Business alignment.
To build an effective foundation for execution, an organization has to pay attention to its operating model, enterprise architecture, and IT engagement model. Such a foundation calls for formulating an IT strategy that aligns with the business strategy, building internal partnerships between IT and business units, and reengineering of IT as a business partner. IT must enable, support, and drive organization growth. Creating or changing the information strategy impacts corporate strategic planning process, organizational structure and power equations, information systems responsibilities, and technology stack.
The first step to having an empowering IT agenda is to recognize the associated cost implications, complexity, and consequences. “Defensive IT” ensures operational reliability while “Offensive IT” helps organizations leapfrog the competition through clever use of emerging technologies and carries an element of risk. Each style has unique governance needs and must be lead by a skilled communicator who can challenge entrenched in-house thinking. An important point to keep in mind is that achieving and sustaining IT-business alignment is difficult and often treacherous.
Health sector in general has been lagging in adopting information technology for a variety of reasons like lack of demonstrated cost effectiveness, interoperability, high adoptions cost, and confidentiality requirements. Some of the challenges are unique to the health industry alone but many are common to industries at large and it may be worthwhile taking lessons from outside of this vertical.
Bringing information strategy into the boardroom makes the organization agile and equips it to respond quickly to a fast changing and evolving market. It brings together motivated experts, empowered decision makers and digitized process. A strategic execution officer or the CIO, under the umbrella of a “Center of Excellence for Innovation and Technology,” could evangelize the need for strategic information management, make IT investment decisions, transition management, and coordinate enterprise change projects.
To build an effective foundation for execution, an organization has to pay attention to its operating model, enterprise architecture, and IT engagement model. Such a foundation calls for formulating an IT strategy that aligns with the business strategy, building internal partnerships between IT and business units, and reengineering of IT as a business partner. IT must enable, support, and drive organization growth. Creating or changing the information strategy impacts corporate strategic planning process, organizational structure and power equations, information systems responsibilities, and technology stack.
The first step to having an empowering IT agenda is to recognize the associated cost implications, complexity, and consequences. “Defensive IT” ensures operational reliability while “Offensive IT” helps organizations leapfrog the competition through clever use of emerging technologies and carries an element of risk. Each style has unique governance needs and must be lead by a skilled communicator who can challenge entrenched in-house thinking. An important point to keep in mind is that achieving and sustaining IT-business alignment is difficult and often treacherous.
Health sector in general has been lagging in adopting information technology for a variety of reasons like lack of demonstrated cost effectiveness, interoperability, high adoptions cost, and confidentiality requirements. Some of the challenges are unique to the health industry alone but many are common to industries at large and it may be worthwhile taking lessons from outside of this vertical.
Bringing information strategy into the boardroom makes the organization agile and equips it to respond quickly to a fast changing and evolving market. It brings together motivated experts, empowered decision makers and digitized process. A strategic execution officer or the CIO, under the umbrella of a “Center of Excellence for Innovation and Technology,” could evangelize the need for strategic information management, make IT investment decisions, transition management, and coordinate enterprise change projects.
Thursday, November 25, 2010
Healthcare IT in India - An Optimistic Outlook - Issue 18 - Information Technology - Asian Hospital & Healthcare Management
Challenges in integrating IT into the healthcare system in India are many, but they can be addressed through leadership and vision.
Healthcare IT in India - An Optimistic Outlook - Issue 18 - Information Technology - Asian Hospital & Healthcare Management
Healthcare IT in India - An Optimistic Outlook - Issue 18 - Information Technology - Asian Hospital & Healthcare Management
Revamped Info System revives Delhi Hospital
Sir Ganga Ram Hospital in Delhi has gone on a journey of computerisation for more than two decades. An in-house system was built in the beginning. But it became “terribly dated”, prompting the hospital to adopt a commercially available package Health Information System
Read the full article here on Future Gov India
Read the full article here on Future Gov India
Sunday, November 21, 2010
Union Budget 2010-11 Roadmap for Healthcare in India - eHealth Article
Union Budget 2010-11 Roadmap for Healthcare in India - eHealth Article
Healthcare, expected to reach over US$75 billion by 2010 and US$150 billion by 2017, has a huge potential for growth in India.
The link analyses the prospects that the current budget unfolds in terms of financial allocations and policy measures to give a boost to healthcare industry in India.
Healthcare, expected to reach over US$75 billion by 2010 and US$150 billion by 2017, has a huge potential for growth in India.
The link analyses the prospects that the current budget unfolds in terms of financial allocations and policy measures to give a boost to healthcare industry in India.
Healthcare Technology Investments in India
Read this interesting article by following the link below
Kid in a Candy Store
A Springboard press release on Healthcare IT Spending in India
Healthcare IT Spending in India to Grow at 22% from 2009-13, finds Springboard Research
Kid in a Candy Store
A Springboard press release on Healthcare IT Spending in India
Healthcare IT Spending in India to Grow at 22% from 2009-13, finds Springboard Research
Public market research reports for Healthcare Market Research in India
There are some reports available in the public domain (Members only access though :-( ). Links to premium reports are also given in the website. Please follow the link below.
Public market research reports for Healthcare Market Research in India, November 2010
Public market research reports for Healthcare Market Research in India, November 2010
Monday, November 8, 2010
Innovations in Healthcare Management and Innovations
IPQC has some great papers and presentations on the following:
Mobile Healthcare Delivery
e-Health in Asia Pacific
Defining and Testing EMR Usability
Click here to read them. All free IPQC Konwledge Center
Enjoy the read
Mobile Healthcare Delivery
e-Health in Asia Pacific
Defining and Testing EMR Usability
Click here to read them. All free IPQC Konwledge Center
Enjoy the read
Monday, October 18, 2010
Health Reform Timeline
Implementation Timeline
The implementation timeline is an interactive tool designed to explain how and when the provisions of the health reform law will be implemented over the next several years.
Timeline @ KFF
The implementation timeline is an interactive tool designed to explain how and when the provisions of the health reform law will be implemented over the next several years.
Timeline @ KFF
The EHR Life Cycle: HIM's Role in the Metamorphosis From Paper
This is a good overview on some of the challenges of implementing EMR solution.
The EHR Life Cycle: HIM's Role in the Metamorphosis From Paper
The EHR Life Cycle: HIM's Role in the Metamorphosis From Paper
Sunday, October 17, 2010
Meaningful Use
The Definition of Meaningful Use Requirements
The requirements of meaningful use to qualify for incentive payments was released on July 13, 2010. The final rule definitively outlines all the specifics of Stage 1 meaningful use and clinical quality measure reporting to receive the incentive payments in 2011 and 2012.
The Recovery Act specifies three main components of Meaningful Use:
The use of a certified EHR in a meaningful manner (e.g.: e-Prescribing);
The use of certified EHR technology for electronic exchange of health information to improve quality of health care; and
The use of certified EHR technology to submit clinical quality and other measures.
The definition of meaningful use harmonizes criteria across CMS programs as much as possible and coordinate with existing CMS quality initiatives. It also closely links to the certification standards criteria in development by the Office of the National Coordinator (ONC) and provides a platform for a staged implementation over time.
Specifics of Stage 1 Meaningful Use (2011 and 2012)
Meaningful use includes both a core set and a menu set of objectives that are specific for eligible professionals and hospitals. For Eligible Professionals, there are a total of 25 meaningful use objectives. 20 of the objectives must be completed to qualify for an incentive payment. 15 are core objectives that are required, and the remaining 5 objectives may be chosen from the list of 10 menu set objectives. For Hospitals, there are a total of 24 meaningful use objectives. 14 are core objectives that are required, and the remaining 5 objectives may be chosen from the list of 10 menu set objectives.
The definition of meaningful use includes reporting of clinical quality measures. See the link titled "Meaningful Use Clinical Quality Measures" in the Links Inside CMS section below to learn more about these specifications for eligible professionals and hospitals. More information on the final rule and fact sheets regarding meaningful use are available below.
To realize improved health care quality, efficiency and patient safety, the criteria for meaningful use will be staged in three steps over the course of the next five years. Stage 1 sets the baseline for electronic data capture and information sharing. Stage 2 (est. 2013) and Stage 3 (est. 2015) will continue to expand on this baseline and be developed through future rule making.
Incentive Program
Core and Menu Set
The requirements of meaningful use to qualify for incentive payments was released on July 13, 2010. The final rule definitively outlines all the specifics of Stage 1 meaningful use and clinical quality measure reporting to receive the incentive payments in 2011 and 2012.
The Recovery Act specifies three main components of Meaningful Use:
The use of a certified EHR in a meaningful manner (e.g.: e-Prescribing);
The use of certified EHR technology for electronic exchange of health information to improve quality of health care; and
The use of certified EHR technology to submit clinical quality and other measures.
The definition of meaningful use harmonizes criteria across CMS programs as much as possible and coordinate with existing CMS quality initiatives. It also closely links to the certification standards criteria in development by the Office of the National Coordinator (ONC) and provides a platform for a staged implementation over time.
Specifics of Stage 1 Meaningful Use (2011 and 2012)
Meaningful use includes both a core set and a menu set of objectives that are specific for eligible professionals and hospitals. For Eligible Professionals, there are a total of 25 meaningful use objectives. 20 of the objectives must be completed to qualify for an incentive payment. 15 are core objectives that are required, and the remaining 5 objectives may be chosen from the list of 10 menu set objectives. For Hospitals, there are a total of 24 meaningful use objectives. 14 are core objectives that are required, and the remaining 5 objectives may be chosen from the list of 10 menu set objectives.
The definition of meaningful use includes reporting of clinical quality measures. See the link titled "Meaningful Use Clinical Quality Measures" in the Links Inside CMS section below to learn more about these specifications for eligible professionals and hospitals. More information on the final rule and fact sheets regarding meaningful use are available below.
To realize improved health care quality, efficiency and patient safety, the criteria for meaningful use will be staged in three steps over the course of the next five years. Stage 1 sets the baseline for electronic data capture and information sharing. Stage 2 (est. 2013) and Stage 3 (est. 2015) will continue to expand on this baseline and be developed through future rule making.
Incentive Program
Core and Menu Set
Tuesday, October 5, 2010
Revisiting HL7
The term HL7 may be used in a number of contexts and it may be worthwhile to know a little about it. I have tried to cull information from various places and put it down in a few brief passages.
HL7 is represents "global standards for the exchange, management and integration of data that supports clinical patient care and the management, delivery and evaluation of healthcare services." It also stands for the (HL7) group that is a Designated Standards Maintenance Organization comprised of healthcare providers, software vendors and consultants.
The initial Version 2 of HL7 was message based and built more or less in an ad hoc manner.HL7 V2.x focused mainly on the "syntax" (structure and layout) for communication between systems.
The Version 3 is model-based built upon the Reference Information Model (RIM)
Version 3 is object-oriented (meaning that it combines data structures with functions to create re-usable objects).RIM is a unique representation of the health care domain set of information and data. RIM represents the semantic and lexical connections between the information carried in the fields of HL7 messages. RIM provides the basis for creating HIS application architecture and persistence layers. There is a RIM implementation based on Java that is available.
HL7 version 3 specifications37 for RIM include:
- Nouns--things that are being communicated
- Adjectives--descriptors and relationships of the nouns
- Verbs--actions being requested or communicated
- semantics of the communication--the actual meaning of a message
- syntax for communication--the structure and layout of the communication
- A channel to carry the communication
On a technical level, RIM is a collection of:
- Subject areas
- Classes--a template which defines the variables and methods for a particular type of object, example: patient class. Core RIM classes are Entity, Role, Participation, Act, Act-Relationship and Role-Link.
- Attributes--qualities of a class, for instance patient class would have name, date of birth, sex, address, etc.39
- Use cases--a way in which a system can be used, described as a step-by-step sequence of actions, along with the system's response and certain other information
- Actors--patients, medical and health professionals, and anyone else involved in a health care event
- Trigger events, example: follow-up clinical visit by a patient
Interactions
For clinical content needs, the HL7 vocabulary tables refer to external terminology sources like SNOMED, ICD10.
Detailed RIM tutorials @ are here
EHR, itself being a repository if information, does not have a standard. But HL7 drafted a functional model for EHR systems. The model helps create functional profiles. The profiles are listed below
Direct Care Profile
- Care Management
- Clinical Decision Support
- Operations Management and Communication
Supportive Profile
- Clinical Support
- Measurement, Analysis, Reporting, Research
- Administrative and Financial
Information Infrastructure Profile
- EHR Security
- EHR Information and Records Management
- Unique Identity, Registry and Directory services
- Support for HIT standards
- Interoperability
- Manage Business Rules
- Workflows
In total there are about 125 functions each with a function name, function statement, description and rationale for inclusion.
The clinical domains include
– Laboratory, Radiology, Nursing, Surgery, Pharmacy, Dietary
Administrative domains include…
– Registration, Billing, Scheduling, Medical records, Staff demographics
– Authorization and permissions
In an effort to create a Healthcare Business Process Reference Model, we can use the HL7 Healthcare Development Framework's practices. One practice that interested me in particular is the Domain Analysis. The diagram below gives the structure of accomplishing a typical domain analysis.

In summary, there is much to be leveraged from HL7 artifacts but finding what is relevant in an ocean of artifacts is a challenge :-).
HL7 is represents "global standards for the exchange, management and integration of data that supports clinical patient care and the management, delivery and evaluation of healthcare services." It also stands for the (HL7) group that is a Designated Standards Maintenance Organization comprised of healthcare providers, software vendors and consultants.
The initial Version 2 of HL7 was message based and built more or less in an ad hoc manner.HL7 V2.x focused mainly on the "syntax" (structure and layout) for communication between systems.
The Version 3 is model-based built upon the Reference Information Model (RIM)
Version 3 is object-oriented (meaning that it combines data structures with functions to create re-usable objects).RIM is a unique representation of the health care domain set of information and data. RIM represents the semantic and lexical connections between the information carried in the fields of HL7 messages. RIM provides the basis for creating HIS application architecture and persistence layers. There is a RIM implementation based on Java that is available.
HL7 version 3 specifications37 for RIM include:
- Nouns--things that are being communicated
- Adjectives--descriptors and relationships of the nouns
- Verbs--actions being requested or communicated
- semantics of the communication--the actual meaning of a message
- syntax for communication--the structure and layout of the communication
- A channel to carry the communication
On a technical level, RIM is a collection of:
- Subject areas
- Classes--a template which defines the variables and methods for a particular type of object, example: patient class. Core RIM classes are Entity, Role, Participation, Act, Act-Relationship and Role-Link.
- Attributes--qualities of a class, for instance patient class would have name, date of birth, sex, address, etc.39
- Use cases--a way in which a system can be used, described as a step-by-step sequence of actions, along with the system's response and certain other information
- Actors--patients, medical and health professionals, and anyone else involved in a health care event
- Trigger events, example: follow-up clinical visit by a patient
Interactions
For clinical content needs, the HL7 vocabulary tables refer to external terminology sources like SNOMED, ICD10.
Detailed RIM tutorials @ are here
EHR, itself being a repository if information, does not have a standard. But HL7 drafted a functional model for EHR systems. The model helps create functional profiles. The profiles are listed below
Direct Care Profile
- Care Management
- Clinical Decision Support
- Operations Management and Communication
Supportive Profile
- Clinical Support
- Measurement, Analysis, Reporting, Research
- Administrative and Financial
Information Infrastructure Profile
- EHR Security
- EHR Information and Records Management
- Unique Identity, Registry and Directory services
- Support for HIT standards
- Interoperability
- Manage Business Rules
- Workflows
In total there are about 125 functions each with a function name, function statement, description and rationale for inclusion.
The clinical domains include
– Laboratory, Radiology, Nursing, Surgery, Pharmacy, Dietary
Administrative domains include…
– Registration, Billing, Scheduling, Medical records, Staff demographics
– Authorization and permissions
In an effort to create a Healthcare Business Process Reference Model, we can use the HL7 Healthcare Development Framework's practices. One practice that interested me in particular is the Domain Analysis. The diagram below gives the structure of accomplishing a typical domain analysis.

In summary, there is much to be leveraged from HL7 artifacts but finding what is relevant in an ocean of artifacts is a challenge :-).
Friday, September 24, 2010
India HIT case study
India HIT case study
Despite India’s recent ascendancy as the hub of the IT and IT-enabled services industry powered by a
vast pool of skilled manpower, it has lagged tremendously behind other countries in HIT adoption. Large
corporate hospitals in India spend under 1% of their operating budget on IT, while spending is closer to
3% in the West. Barring a few preliminary attempts to computerize basic hospital administrative and some
clinical functions, there has been little appreciation or impetus given to HIT adoption.
Despite India’s recent ascendancy as the hub of the IT and IT-enabled services industry powered by a
vast pool of skilled manpower, it has lagged tremendously behind other countries in HIT adoption. Large
corporate hospitals in India spend under 1% of their operating budget on IT, while spending is closer to
3% in the West. Barring a few preliminary attempts to computerize basic hospital administrative and some
clinical functions, there has been little appreciation or impetus given to HIT adoption.
PWC report on Healthcare in India
PWC report on Healthcare in India
Healthcare is one of India’s largest sectors, in terms of revenue and
employment, and the sector is expanding rapidly. During the 1990s, Indian
healthcare grew at a compound annual rate of 16%. Today the total value
of the sector is more than $34 billion. This translates to $34 per capita,
or roughly 6% of GDP. By 2012, India’s healthcare sector is projected to
grow to nearly $40 billion.
The private sector accounts for more than 80% of total healthcare
spending in India. Unless there is a decline in the combined federal and
state government deficit, which currently stands at roughly 9%, the
opportunity for significantly higher public health spending will be limited
Healthcare is one of India’s largest sectors, in terms of revenue and
employment, and the sector is expanding rapidly. During the 1990s, Indian
healthcare grew at a compound annual rate of 16%. Today the total value
of the sector is more than $34 billion. This translates to $34 per capita,
or roughly 6% of GDP. By 2012, India’s healthcare sector is projected to
grow to nearly $40 billion.
The private sector accounts for more than 80% of total healthcare
spending in India. Unless there is a decline in the combined federal and
state government deficit, which currently stands at roughly 9%, the
opportunity for significantly higher public health spending will be limited
Friday, August 6, 2010
Healthcare Quality Organizations
The the following are excerpts from an article by my friend Joshua Chu (MS Healthcare Management University of Texas Dallas)
American Healthcare Accreditation
In the United States, most hospitals are accredited through an organization that is known as the Joint Commission. Joint Commission accreditation holds a significant stake within the healthcare system in that it controls Medicaid reimbursements. Joint Commission is a nonprofit organization, operated by volunteers. This is the aspiration of the men and women of Joint Commission: Their mission is "To continuously improve health care for the public, in collaboration with other stakeholders, by evaluating health care organizations and inspiring them to excel in providing safe and effective care of the highest quality and value.” (4)
The organization of Joint Commission came from humble beginnings when Earnest Codman began to promote reforms in hospitals to be compensated financially based on the quality of performance outcome in patient care. Thus, the American College of Surgeons Hospital Standardization Program was born, being the first healthcare quality entity to be wide spread across the nation.
The way that Joint Commission works is that they have a three year cycle in which hospitals are inspected in intervals to gain Joint Commission’s accreditation. During this time, the hospital will be inspected to see if it meets all the requirements of accomplishing compliance with applicable standards. When a hospital does meet their demands, they will be awarded accreditation.
The unique part of Joint Commission’s inspection is that their surveys are surprised and unannounced. As such, hospitals are encouraged to be in top performance in order to avoid losing their accreditation. This has the effect of improving consistency for performance of hospitals that receives accreditation from Joint Commission. Another part about their accreditation is that it is mainly on a pass/fail basis, where the findings of the surveyor is not published and the public will only know whether the hospital was able to acquire their accreditation or not.
As of today, Joint Commission has expanded into the Joint Commission International, where they are still operating as a nonprofit organization with the goal and mission to improve patient quality care worldwide. They extended their influence and offer to help improve the quality of hospitals and enhance patient safety across the globe.
Despite the fact that Joint Commission is the significant portion of American Hospital accreditation, it is not a monopoly and that many alternatives do exist, but not as to the same extent. The fact that Joint Commission is the standard of how the U.S. government decides on which hospital to approve for Medicaid reimbursement has significant influence of the accreditation market.
An example of an alternative accreditation to Joint Commission which is recognized nationwide is the Healthcare Facilities Accreditation Program, which was founded in 1943, making the organization older than Joint Commission. The organization was quickly able to gain recognition, and by the mid 1960s, the United States Congress decided that hospitals being accredited by this group were qualified to participate in the Medicare and Medicaid Programs. Their organizational goals are not so different from Joint Commission in that they desire to help healthcare facilities which are under their accreditation deliver high quality patient care by means of meeting the standards set by the organization. They are committed to continuous improvement through the constant review and streamlining of their survey processes.
International Healthcare Accreditation
The desire for quality within the medical community is not exclusive to America. This fact factored along with growing trend towards globalization and medical tourism, there is significant interests in international accreditation of hospitals. Joint Commission is one of those examples, having already grown beyond the borders of America. They have established themselves across over 60 other countries around the world. This trend is more prevalent within the developed world where growing consumerism culture is making the patients, otherwise known as the consumers, more conscious of the care that they are given, or in the other terms, services given. As such, quality assurance is a critical part of the value chain of a healthcare provider and is not unique to the United States.
Healthcare delivery has always been defined by three distinct pillars. They are availability, cost, and quality. In much of the European Union, availability and cost of their healthcare systems has been relatively well managed. Thus, many Europeans are now looking towards quality as the next challenge to tame. This is evident as the Office of Public Health and Social Affairs stated, “... patients have ever-greater expectations of what health systems ought to deliver,” although there has been a “... continuous rise in costs of services determined by scientific and technological innovation.”(2) Healthcare being available in many countries around the world, it is imperative for these institutions to also deliver on quality. This is not only serving more people but also saving more people in the end.
Another issue that has lead to greater interest in international accreditation has been more closely tied into the new trend of Global Healthcare. As our world begins to get smaller and traveling becomes more and more easy, the law of economics and sociology only dictates that humans will ultimately seek out the sources of highest output for the lowest cost. And in this case, healthcare is no exception to this rule. Thus, we see more and more Americans traveling overseas for Medical Tourism and vice versa. Many people around the world also travel to the United States for treatment due to long established specialty. It is no easy decision for any individual, however, for such a trip takes time and commitment. We are seeing a new generation of patients who will do much greater research to find the best solutions to their problems. In order for overseas hospitals to get the patients there for medical tourism, they must have two advantages which will ultimately prompt the patient to travel to them. In this instance, the two factors include cost and quality. With the deficit in healthcare ever increasing in the United States, healthcare affordability has become a much heated issue. This factored in with the recent economic down turn, many people in the United States remain uninsured due to the costs issue. An attractive option will present to this group through the address of their problems with money. These hospitals will a lot of times be able to deliver care in a much more efficient manner due to cheaper infrastructure and support cost, thus the savings are given back to the customer. When the entire operation cost results in a price tag cheaper than what the patient would have to pay for in deductibles, this is usually good enough bait to lure in a customer. However, cost itself is not good enough to attract a customer. The question of quality has to be addressed, as not many people would be willing to take risks to their lives all in the name of costs alone. This is where international accreditation comes in. They can assure to the customers around the world that the hospitals standards within other nations are the same, if not better, than the quality of hospitals they have at home. With these two issues addressed, often times many people will then be willing travel to get healthcare at Great Value. Quality without addressing would not work simply because most consumers cannot afford them and will be seen as an activity that is overpriced. On the other hand, cost without quality will also be unacceptable, for patients will only be gambling their lives to save money. Only with the two pillars addressed will patients be willing to travel, and with international accreditation, many patients across the globe have a quality standard of these Medical Tourist Hospitals that they can relate to and are familiar with since they are the same accreditation at home.
So what is international accreditation exactly? In many developed nations around the world, hospital accreditation has been in the making internally for time now. An example would be Joint Commission within the United States. As such, many older nations have naturally become the guru of quality in the healthcare industry, setting the bar for others to follow. For an example, recently, China has begun on their set of healthcare reforms. When it came to the topic of quality, they used the United States accreditation standards as a precedence for which they can set and work with. (3) As such, accreditation standards used here in the United States are being used by foreign countries to access their own healthcare systems. Therefore, many new prosperous nations seek the services of major international healthcare accreditation group in order to bring their own hospitals up to the global standards. Aside from improvement of quality service to their own citizens among these countries that have seek international accreditation, they also seek the accreditation on the basis of quality assurance to medical tourists, hoping to market themselves better in the process and attract more medical tourists to their facilities. This will secure their competitive advantage to better deliver care as well. Many foreign governments are getting into the game also due to the fact that medical tourism is becoming a huge industry among these countries bringing in revenue and growth to their economy in the process. As such, international accreditation will enable them to better market themselves to foreign citizens and attract them thus fueling the growth of their own healthcare industries within their perspective borders.
International Healthcare Accreditation Agencies
As a result of increasing demand of accreditation, the Trent Accreditation Scheme came into the expansionist policy that it is right now. Based in the United Kingdom, it was the accreditation force behind much of the hospital systems within the nation and for her colonies. As a result, as England began losing control over much of their former colonies, the Trent Accreditation Scheme still remained as a huge player in many of those countries, including former colonies of the crown in Asia specifically Hong Kong. As such, the organization was pushed into the international stage.
Joint Commission International is a group that we are all familiar with. Recently, it has expanded to well over 60 other countries around the world, and through it international accreditation activities in many countries, it would bring an income to the parent company of Joint Commission which is based in the United States. This would further show how high the demand is for hospitals around the world to be recognized as on par with American hospitals thus being able to compete for patients to enter into their market.
The International Society for Quality in Health Care is an accreditation organization that operates as an umbrella organization for its accreditation groups across the globe. Being based in Ireland, the group operates as primarily a consulting group that would further the quality of healthcare of the hospitals that they are working with. (5)
The Government as a Healthcare Quality Control Entity
With such significant profound effect on the population of any society that health care have, government is definitely a significantly important stake holder. As such, a lot of times, government would demand quality from healthcare providers so that the patients going through those hospitals will get better and not worse and the way that government influence healthcare quality is by means of laws, legislations and rewarding of reimbursements.
An example of legislation that has an effect on quality care and patient safety is the Patient Safety and Quality Improvement Act that was passed in 2005. (5) Through this bill, it established a system of patient safety organizations in order to encourage the discussion of case complications and how to avoid them.
The legislation is attributed as a response to the publication of “To Err is Human” by the Institute of Medicine 1999 report. Within this report it points to the staggering numbers that medical errors have on people. The report’s finding suggests that most errors are not the result of human error, but as the result of error within the process, an error that can be fixed by administrative diligence. Therefore, the report recommend that administration on all levels work together to improve safety making it harder for all levels within the system to make a mistake while making it easier to avoid preventable errors.
Other initiative including bargaining power that the government has in the forms of reimbursements control where hospitals have to be eligible for them, and as a result, giving rise to powers such as Joint Commission, where the government will not qualify a hospital unless they have accreditation from Joint Commission or one of their major competitive alternatives.
BIBLIOGRAPHY
1. Raik, Eva. "Bmj.com Rapid Responses for Braithwaite, 323 (7310) 443-446." Bmj.com:. Aged Care Accreditation in Australia, 7 Nov. 2001. Web. 02 July 2010..
2. "Contribution to the Reflection Process for a New EU Health Strategy." Venice Italy: Regional Health and Social Department, Web. 06 July 2010..
3. Lipson, Roberta. "Investing in China's Hospitals -- CBR Nov-Dec 2004." The China Business Review: The Magazine of the US-China Business Council. Web. 03 July 2010..
4. "Facts about The Joint Commission | Joint Commission." The Joint Commission. Joint Commission. Web. 13 Nov. 2009..
5. "International Society for Quality in Health Care Inc, Accreditation." International Society for Quality in Health Care Ltd. Web. 01 Aug. 2010.
6. Six Sigma Job: Master Black Belt/Six Sigma Consultant- Telecommut." I Six Sigma Job Shop - Six Sigma Jobs. Web. 02 Aug. 2010..
American Healthcare Accreditation
In the United States, most hospitals are accredited through an organization that is known as the Joint Commission. Joint Commission accreditation holds a significant stake within the healthcare system in that it controls Medicaid reimbursements. Joint Commission is a nonprofit organization, operated by volunteers. This is the aspiration of the men and women of Joint Commission: Their mission is "To continuously improve health care for the public, in collaboration with other stakeholders, by evaluating health care organizations and inspiring them to excel in providing safe and effective care of the highest quality and value.” (4)
The organization of Joint Commission came from humble beginnings when Earnest Codman began to promote reforms in hospitals to be compensated financially based on the quality of performance outcome in patient care. Thus, the American College of Surgeons Hospital Standardization Program was born, being the first healthcare quality entity to be wide spread across the nation.
The way that Joint Commission works is that they have a three year cycle in which hospitals are inspected in intervals to gain Joint Commission’s accreditation. During this time, the hospital will be inspected to see if it meets all the requirements of accomplishing compliance with applicable standards. When a hospital does meet their demands, they will be awarded accreditation.
The unique part of Joint Commission’s inspection is that their surveys are surprised and unannounced. As such, hospitals are encouraged to be in top performance in order to avoid losing their accreditation. This has the effect of improving consistency for performance of hospitals that receives accreditation from Joint Commission. Another part about their accreditation is that it is mainly on a pass/fail basis, where the findings of the surveyor is not published and the public will only know whether the hospital was able to acquire their accreditation or not.
As of today, Joint Commission has expanded into the Joint Commission International, where they are still operating as a nonprofit organization with the goal and mission to improve patient quality care worldwide. They extended their influence and offer to help improve the quality of hospitals and enhance patient safety across the globe.
Despite the fact that Joint Commission is the significant portion of American Hospital accreditation, it is not a monopoly and that many alternatives do exist, but not as to the same extent. The fact that Joint Commission is the standard of how the U.S. government decides on which hospital to approve for Medicaid reimbursement has significant influence of the accreditation market.
An example of an alternative accreditation to Joint Commission which is recognized nationwide is the Healthcare Facilities Accreditation Program, which was founded in 1943, making the organization older than Joint Commission. The organization was quickly able to gain recognition, and by the mid 1960s, the United States Congress decided that hospitals being accredited by this group were qualified to participate in the Medicare and Medicaid Programs. Their organizational goals are not so different from Joint Commission in that they desire to help healthcare facilities which are under their accreditation deliver high quality patient care by means of meeting the standards set by the organization. They are committed to continuous improvement through the constant review and streamlining of their survey processes.
International Healthcare Accreditation
The desire for quality within the medical community is not exclusive to America. This fact factored along with growing trend towards globalization and medical tourism, there is significant interests in international accreditation of hospitals. Joint Commission is one of those examples, having already grown beyond the borders of America. They have established themselves across over 60 other countries around the world. This trend is more prevalent within the developed world where growing consumerism culture is making the patients, otherwise known as the consumers, more conscious of the care that they are given, or in the other terms, services given. As such, quality assurance is a critical part of the value chain of a healthcare provider and is not unique to the United States.
Healthcare delivery has always been defined by three distinct pillars. They are availability, cost, and quality. In much of the European Union, availability and cost of their healthcare systems has been relatively well managed. Thus, many Europeans are now looking towards quality as the next challenge to tame. This is evident as the Office of Public Health and Social Affairs stated, “... patients have ever-greater expectations of what health systems ought to deliver,” although there has been a “... continuous rise in costs of services determined by scientific and technological innovation.”(2) Healthcare being available in many countries around the world, it is imperative for these institutions to also deliver on quality. This is not only serving more people but also saving more people in the end.
Another issue that has lead to greater interest in international accreditation has been more closely tied into the new trend of Global Healthcare. As our world begins to get smaller and traveling becomes more and more easy, the law of economics and sociology only dictates that humans will ultimately seek out the sources of highest output for the lowest cost. And in this case, healthcare is no exception to this rule. Thus, we see more and more Americans traveling overseas for Medical Tourism and vice versa. Many people around the world also travel to the United States for treatment due to long established specialty. It is no easy decision for any individual, however, for such a trip takes time and commitment. We are seeing a new generation of patients who will do much greater research to find the best solutions to their problems. In order for overseas hospitals to get the patients there for medical tourism, they must have two advantages which will ultimately prompt the patient to travel to them. In this instance, the two factors include cost and quality. With the deficit in healthcare ever increasing in the United States, healthcare affordability has become a much heated issue. This factored in with the recent economic down turn, many people in the United States remain uninsured due to the costs issue. An attractive option will present to this group through the address of their problems with money. These hospitals will a lot of times be able to deliver care in a much more efficient manner due to cheaper infrastructure and support cost, thus the savings are given back to the customer. When the entire operation cost results in a price tag cheaper than what the patient would have to pay for in deductibles, this is usually good enough bait to lure in a customer. However, cost itself is not good enough to attract a customer. The question of quality has to be addressed, as not many people would be willing to take risks to their lives all in the name of costs alone. This is where international accreditation comes in. They can assure to the customers around the world that the hospitals standards within other nations are the same, if not better, than the quality of hospitals they have at home. With these two issues addressed, often times many people will then be willing travel to get healthcare at Great Value. Quality without addressing would not work simply because most consumers cannot afford them and will be seen as an activity that is overpriced. On the other hand, cost without quality will also be unacceptable, for patients will only be gambling their lives to save money. Only with the two pillars addressed will patients be willing to travel, and with international accreditation, many patients across the globe have a quality standard of these Medical Tourist Hospitals that they can relate to and are familiar with since they are the same accreditation at home.
So what is international accreditation exactly? In many developed nations around the world, hospital accreditation has been in the making internally for time now. An example would be Joint Commission within the United States. As such, many older nations have naturally become the guru of quality in the healthcare industry, setting the bar for others to follow. For an example, recently, China has begun on their set of healthcare reforms. When it came to the topic of quality, they used the United States accreditation standards as a precedence for which they can set and work with. (3) As such, accreditation standards used here in the United States are being used by foreign countries to access their own healthcare systems. Therefore, many new prosperous nations seek the services of major international healthcare accreditation group in order to bring their own hospitals up to the global standards. Aside from improvement of quality service to their own citizens among these countries that have seek international accreditation, they also seek the accreditation on the basis of quality assurance to medical tourists, hoping to market themselves better in the process and attract more medical tourists to their facilities. This will secure their competitive advantage to better deliver care as well. Many foreign governments are getting into the game also due to the fact that medical tourism is becoming a huge industry among these countries bringing in revenue and growth to their economy in the process. As such, international accreditation will enable them to better market themselves to foreign citizens and attract them thus fueling the growth of their own healthcare industries within their perspective borders.
International Healthcare Accreditation Agencies
As a result of increasing demand of accreditation, the Trent Accreditation Scheme came into the expansionist policy that it is right now. Based in the United Kingdom, it was the accreditation force behind much of the hospital systems within the nation and for her colonies. As a result, as England began losing control over much of their former colonies, the Trent Accreditation Scheme still remained as a huge player in many of those countries, including former colonies of the crown in Asia specifically Hong Kong. As such, the organization was pushed into the international stage.
Joint Commission International is a group that we are all familiar with. Recently, it has expanded to well over 60 other countries around the world, and through it international accreditation activities in many countries, it would bring an income to the parent company of Joint Commission which is based in the United States. This would further show how high the demand is for hospitals around the world to be recognized as on par with American hospitals thus being able to compete for patients to enter into their market.
The International Society for Quality in Health Care is an accreditation organization that operates as an umbrella organization for its accreditation groups across the globe. Being based in Ireland, the group operates as primarily a consulting group that would further the quality of healthcare of the hospitals that they are working with. (5)
The Government as a Healthcare Quality Control Entity
With such significant profound effect on the population of any society that health care have, government is definitely a significantly important stake holder. As such, a lot of times, government would demand quality from healthcare providers so that the patients going through those hospitals will get better and not worse and the way that government influence healthcare quality is by means of laws, legislations and rewarding of reimbursements.
An example of legislation that has an effect on quality care and patient safety is the Patient Safety and Quality Improvement Act that was passed in 2005. (5) Through this bill, it established a system of patient safety organizations in order to encourage the discussion of case complications and how to avoid them.
The legislation is attributed as a response to the publication of “To Err is Human” by the Institute of Medicine 1999 report. Within this report it points to the staggering numbers that medical errors have on people. The report’s finding suggests that most errors are not the result of human error, but as the result of error within the process, an error that can be fixed by administrative diligence. Therefore, the report recommend that administration on all levels work together to improve safety making it harder for all levels within the system to make a mistake while making it easier to avoid preventable errors.
Other initiative including bargaining power that the government has in the forms of reimbursements control where hospitals have to be eligible for them, and as a result, giving rise to powers such as Joint Commission, where the government will not qualify a hospital unless they have accreditation from Joint Commission or one of their major competitive alternatives.
BIBLIOGRAPHY
1. Raik, Eva. "Bmj.com Rapid Responses for Braithwaite, 323 (7310) 443-446." Bmj.com:. Aged Care Accreditation in Australia, 7 Nov. 2001. Web. 02 July 2010.
2. "Contribution to the Reflection Process for a New EU Health Strategy." Venice Italy: Regional Health and Social Department, Web. 06 July 2010.
3. Lipson, Roberta. "Investing in China's Hospitals -- CBR Nov-Dec 2004." The China Business Review: The Magazine of the US-China Business Council. Web. 03 July 2010.
4. "Facts about The Joint Commission | Joint Commission." The Joint Commission. Joint Commission. Web. 13 Nov. 2009.
5. "International Society for Quality in Health Care Inc, Accreditation." International Society for Quality in Health Care Ltd. Web. 01 Aug. 2010.
6. Six Sigma Job: Master Black Belt/Six Sigma Consultant- Telecommut." I Six Sigma Job Shop - Six Sigma Jobs. Web. 02 Aug. 2010.
Thursday, August 5, 2010
EBM and Data Warehousing
Introduction
Evidence based medicine (EBM) replaces the traditional model of “medicine by authority” with a scientific model that avoids the use of underutilized and unsystematic information [1]. It encourages healthcare professionals and managers to be aware of and make use of published peer research. EBM requires that decisions makers have access to methodically compiled research information. It enhances knowledge and speeds the introduction of new therapies and withdrawal of ineffective ones. Thus, EBM represents a knowledge management system in the world of healthcare. Knowledge comes from information, which results from processing data. In the current age, information come a variety of sources including published scientific and technical literature, clearinghouses for public domain information, and internet. Information technology contributes to EBM in the following ways [2]:
•Reference databases – contains formal publication of clinical trials and reviews. Conventional databases are not usually effective in providing contextual, timely, precise information sought by physicians. However, entities like the Cochrane Collaboration Library do a good job of meeting the clinician criteria [3].
•Contextual and case-specific information – collected from current and past encounters with the healthcare system. Usually it consists of transaction data with the insurance provider and health provider’s administrative information system. It also accounts from the epidemiological and social factors for a particular site [4].
•Clinical and administrative data repositories – Data captured at the point of care through hospital information systems and electronic medical records
•Decision support software – Creation of clear and reproducible rules to facilitate clinical decision making
•Internet based interactive health information – Contains multimedia resources, unstructured content, unendorsed, and non-validated data.
EBM Data Warehouse cardinality
Evidence based medicine needs the support of organizations that provide means to search, store, and retrieve contextual patient relevant data to the clinician in a timely manner. This translates to the creation of a place where data is constantly maintained and updated, classified and populated to study variables uniformly under a nosological or classification system [5]. Using various data mining techniques the medical community can understand patterns of care, causal pathways, profile best practices, and create benchmarks. According to Kimble and Inmon (1996), the DW is Subject-Oriented, Integrated, Time-Variant, Non-Volatile data in support of management decisions. Data warehouse is also not only a product or a collection of subsystems, but also a process. The following table shows the relationship between
EBM functions and data warehouse
EBM feature------------------------------>Data Warehouse feature
A diagnosis needs to be established------>Query
A therapy mode or care pathways needs
to be determined------------------------->Query
A prognosis is needed-------------------->Prediction
Possible causes need to be verified------>Pattern recognition
An Architectural proposition
For the remainder of the paper, we will discuss the data warehouse part of the EBM criteria. Using the corporate information factory model [7] (Refer to illustration A) as a baseline, a nationally managed central enterprise data warehouse is not a feasible solution. EBM needs the following
•Information integration from heterogeneous systems
Today, several repositories and data marts exist within the boundaries of institutions. The critical success factor is to have them share the data keeping in mind the questions of privacy, software regulation, and ethical and legal aspects of telecommunication in healthcare.
Neutral standards like Simple Object Access Protocol (SOAP) combined with Service oriented architecture framework provide a paradigm to integrate information seamlessly
•Standardized facades for information exchange
The single most important factor in information integration is the contract for information exchange. All institutions need to model their repositories off a reference implementation, which will have a skeletal, minimal set of fact and dimension tables like Patient, Clinic, Clinician, Drug, Therapy, Diagnosis, Prescription, and Encounter [8].
From a governance standpoint, key stakeholders of medical data repositories must be accountable to participate in scheme of Electronic Health Record (EHR). EHR lays the foundation for inter institutional exchange of clinical data.
•A nationally managed online gateway to a network of repositories
Bill Inmon defines this as a “virtual DW” which has the ability to farm out a query serviced in parallel by two or more distributed databases, aggregate and join results from those databases, and deliver a unified result set to the requester.
Hurdles
There are “hard” and “soft” hurdles for data warehouse based EBM. Some of them are below:
•Complex nature of the of the care delivery which includes interdependence of staff skills, clinical equipment, patient risks, guidelines and drugs and possibly other factors (Refer to illustration B)
•Need for continuous assessment of data warehouse rules and reconciling the outcomes and metrics with the medical advisory committee. This is a labor-intensive task.
•Need to alter physician mind mindset regarding EBM as cookbook medicine
•High volume of data and intricate integration needs bring forth technology and governance challenges.
Conclusions
Even if a national EBM program is technically available, getting the healthcare community to use it, is different matter altogether. Branded as cookbook medicine, health professionals feel that EBM will curtail their individual autonomy to practice. To the hospitals, the patient is market share and sharing patient information is counter intuitive. The patient is worried about privacy issues. Evidence based Practice Center program launched by the Agency for Healthcare Quality and Research has identified organizations to participate in its program. It has identified the priority conditions like cancer, diabetes, dementia, Ischemic heart disease, stroke, and hypertension to name a few. With the introduction of the new “meaningful use guideline” electronic data collection will be faster. The key to effective use of EBM rests on the ability to integrate disparate silos of knowledge built so far. Some of the recommended steps for major health and insurance providers would be to follow standards for information exchange, allow information query, mask patient identifiable information, create new data mart provide wrappers for existing ones, create IT governance organization, and create compliance programs. There is cost considerations involved in participating in these programs. As new incentives emerge for knowledge sharing and as technology-costs continue to come down, medical data warehousing or EBM will move closer to being a practical and viable solution.
References
[1] Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to teaching the practice of medicine. Journal of the American Medical Association, 1992, 268: 2420–2425.
[2] Information systems: the key to evidence-based health practice. Roberto J. Rodrigues. Bulletin of the World Health Organization, 2000, 78 (11)
[3] The Cochrane Collaboration. Valuable resource for family physicians. Becker L. Canadian Family Physician, 1997, 43: 403–404, 412–414.
[4] Enkin MW, Jadad AR. Using anecdotal information in evidence-based health care: heresy or necessity? Annals of Oncology, 1998, 9: 963–966.
[5] Healthcare Informatics Research: From Data to Evidence-Based Management Thomas T. H. Wan Received: 25 March 2005 / Springer Science + Business Media, Inc. 2006
[6] Kimball. R. and Inmon, W.H. (1996). The Data Warehouse Toolkit. John Wiley: New York
[7] Corporate Information Factory. Bill Immon. http://www.inmoncif.com/library/cif/
[8] Towards a sustainable data warehouse for evidence based medicine.Vienna University of Technology, Nevena Stolba
[9] The relevance of data warehousing and data mining in the field of evidence-based medicine to support healthcare decision making. Nevena Stolba and A Min Tjoa
[10] Sen, A. and Sinha, A. P. (2005): A Comparison of Datawarehousing Methodologies, Communication of the ACM, 48(3), 79-84
Evidence based medicine (EBM) replaces the traditional model of “medicine by authority” with a scientific model that avoids the use of underutilized and unsystematic information [1]. It encourages healthcare professionals and managers to be aware of and make use of published peer research. EBM requires that decisions makers have access to methodically compiled research information. It enhances knowledge and speeds the introduction of new therapies and withdrawal of ineffective ones. Thus, EBM represents a knowledge management system in the world of healthcare. Knowledge comes from information, which results from processing data. In the current age, information come a variety of sources including published scientific and technical literature, clearinghouses for public domain information, and internet. Information technology contributes to EBM in the following ways [2]:
•Reference databases – contains formal publication of clinical trials and reviews. Conventional databases are not usually effective in providing contextual, timely, precise information sought by physicians. However, entities like the Cochrane Collaboration Library do a good job of meeting the clinician criteria [3].
•Contextual and case-specific information – collected from current and past encounters with the healthcare system. Usually it consists of transaction data with the insurance provider and health provider’s administrative information system. It also accounts from the epidemiological and social factors for a particular site [4].
•Clinical and administrative data repositories – Data captured at the point of care through hospital information systems and electronic medical records
•Decision support software – Creation of clear and reproducible rules to facilitate clinical decision making
•Internet based interactive health information – Contains multimedia resources, unstructured content, unendorsed, and non-validated data.
EBM Data Warehouse cardinality
Evidence based medicine needs the support of organizations that provide means to search, store, and retrieve contextual patient relevant data to the clinician in a timely manner. This translates to the creation of a place where data is constantly maintained and updated, classified and populated to study variables uniformly under a nosological or classification system [5]. Using various data mining techniques the medical community can understand patterns of care, causal pathways, profile best practices, and create benchmarks. According to Kimble and Inmon (1996), the DW is Subject-Oriented, Integrated, Time-Variant, Non-Volatile data in support of management decisions. Data warehouse is also not only a product or a collection of subsystems, but also a process. The following table shows the relationship between
EBM functions and data warehouse
EBM feature------------------------------>Data Warehouse feature
A diagnosis needs to be established------>Query
A therapy mode or care pathways needs
to be determined------------------------->Query
A prognosis is needed-------------------->Prediction
Possible causes need to be verified------>Pattern recognition
An Architectural proposition
For the remainder of the paper, we will discuss the data warehouse part of the EBM criteria. Using the corporate information factory model [7] (Refer to illustration A) as a baseline, a nationally managed central enterprise data warehouse is not a feasible solution. EBM needs the following
•Information integration from heterogeneous systems
Today, several repositories and data marts exist within the boundaries of institutions. The critical success factor is to have them share the data keeping in mind the questions of privacy, software regulation, and ethical and legal aspects of telecommunication in healthcare.
Neutral standards like Simple Object Access Protocol (SOAP) combined with Service oriented architecture framework provide a paradigm to integrate information seamlessly
•Standardized facades for information exchange
The single most important factor in information integration is the contract for information exchange. All institutions need to model their repositories off a reference implementation, which will have a skeletal, minimal set of fact and dimension tables like Patient, Clinic, Clinician, Drug, Therapy, Diagnosis, Prescription, and Encounter [8].
From a governance standpoint, key stakeholders of medical data repositories must be accountable to participate in scheme of Electronic Health Record (EHR). EHR lays the foundation for inter institutional exchange of clinical data.
•A nationally managed online gateway to a network of repositories
Bill Inmon defines this as a “virtual DW” which has the ability to farm out a query serviced in parallel by two or more distributed databases, aggregate and join results from those databases, and deliver a unified result set to the requester.
Hurdles
There are “hard” and “soft” hurdles for data warehouse based EBM. Some of them are below:
•Complex nature of the of the care delivery which includes interdependence of staff skills, clinical equipment, patient risks, guidelines and drugs and possibly other factors (Refer to illustration B)
•Need for continuous assessment of data warehouse rules and reconciling the outcomes and metrics with the medical advisory committee. This is a labor-intensive task.
•Need to alter physician mind mindset regarding EBM as cookbook medicine
•High volume of data and intricate integration needs bring forth technology and governance challenges.
Conclusions
Even if a national EBM program is technically available, getting the healthcare community to use it, is different matter altogether. Branded as cookbook medicine, health professionals feel that EBM will curtail their individual autonomy to practice. To the hospitals, the patient is market share and sharing patient information is counter intuitive. The patient is worried about privacy issues. Evidence based Practice Center program launched by the Agency for Healthcare Quality and Research has identified organizations to participate in its program. It has identified the priority conditions like cancer, diabetes, dementia, Ischemic heart disease, stroke, and hypertension to name a few. With the introduction of the new “meaningful use guideline” electronic data collection will be faster. The key to effective use of EBM rests on the ability to integrate disparate silos of knowledge built so far. Some of the recommended steps for major health and insurance providers would be to follow standards for information exchange, allow information query, mask patient identifiable information, create new data mart provide wrappers for existing ones, create IT governance organization, and create compliance programs. There is cost considerations involved in participating in these programs. As new incentives emerge for knowledge sharing and as technology-costs continue to come down, medical data warehousing or EBM will move closer to being a practical and viable solution.
References
[1] Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to teaching the practice of medicine. Journal of the American Medical Association, 1992, 268: 2420–2425.
[2] Information systems: the key to evidence-based health practice. Roberto J. Rodrigues. Bulletin of the World Health Organization, 2000, 78 (11)
[3] The Cochrane Collaboration. Valuable resource for family physicians. Becker L. Canadian Family Physician, 1997, 43: 403–404, 412–414.
[4] Enkin MW, Jadad AR. Using anecdotal information in evidence-based health care: heresy or necessity? Annals of Oncology, 1998, 9: 963–966.
[5] Healthcare Informatics Research: From Data to Evidence-Based Management Thomas T. H. Wan Received: 25 March 2005 / Springer Science + Business Media, Inc. 2006
[6] Kimball. R. and Inmon, W.H. (1996). The Data Warehouse Toolkit. John Wiley: New York
[7] Corporate Information Factory. Bill Immon. http://www.inmoncif.com/library/cif/
[8] Towards a sustainable data warehouse for evidence based medicine.Vienna University of Technology, Nevena Stolba
[9] The relevance of data warehousing and data mining in the field of evidence-based medicine to support healthcare decision making. Nevena Stolba and A Min Tjoa
[10] Sen, A. and Sinha, A. P. (2005): A Comparison of Datawarehousing Methodologies, Communication of the ACM, 48(3), 79-84
Wednesday, July 7, 2010
Control Charts in healthcare
Control Charts in healthcare
Statistical Process Control is a methodology of statistical analysis used to discover special cause variation in a process. In healthcare, it is used to document that a critical process is in control and alert responsible parties should there be a deviation. A typical control chart is a graphical representation of the quality indicator, as either individual values or calculated subgroups with the data displayed sequentially and time ordered [Refer to illustration 1 in Appendix]. Horizontal lines represent the central tendency (mean), upper and lower control limits typically set at +3 standard deviations from the mean [1]. In this paper, we will list down the types of control charts available and guidelines to interpret it.
Types of Control Charts
In 1920s by Walter Shewhart developed it to improve industrial manufacturing. It first migrated to healthcare in laboratory settings and then into direct patient care applications [2].
There are four commonly used control charts [Refer to illustration 2, 3 in Appendix]. Control are categorized as upper (+) and lower (-).

A process is “in control” when it has the following characteristics [3]:
No points are outside the control limits – the traditional and most popular SPC chart guideline,
The number of points above and below the center line is about the same,
The points seem to fall randomly above and below the center line,
Most points, but not all, are near the centerline, and only a few are close to the control limits.
Evaluating the “patterns in the sample data” using guidelines such as [Refer to illustration 4 in Appendix]:
Eight points in a row above or below the center line
10 of 11 consecutive points above or below the center line
12 of 14 consecutive points above or below the center line
Two of three consecutive points in the outer one-third region between the center line and one of the control limits
Four of five consecutive points in the outer two-thirds region between the centerline and one of the control limits.
Basic Guidelines
In general, in applying statistical process control, we need to delineate the following:
The study and design objectives
Study settings - entire hospital, department etc
Fields of healthcare – anesthesia, pathology etc
Unit of analysis – Clinicians, patient, staff etc
Variables – Oxygen saturation, time to complete etc
Benefits – Impact assessment, quantify process variability etc
However, a number of special issues arise in health care applications of SPC. One of these is the question of what to measure. In health care applications, there is concern and debate about excessive emphasis on outcome metrics and report cards to the detriment of process understanding and improvement. Another issue is the problem of how to aggregate, adjust, and present rate data, used to make decisions [5].
Conclusion
Control charts provide an effective method to visualize data over a specific monitoring period while considering for boundary conditions. Usually the control limits are well within the specification limits for a capable process [Refer to illustration 5 in Appendix]. Continuing use of the control chart helps to check if the corrective action has resulted in an improved process. They allow hospital administrators to have a more engaging conversation with the physicians in the wake of the collected data. When shared between providers, control charts they drive higher standards of care. Patient identification and non-infectious hazards of transfusion are some typical bio-vigilance areas where software process control finds effective application.


References
[1] Continuous quality improvement of perfusion practice. The role of electronic data collection and statistical control chart. RA Baker, RF Newland. Perfusion 2008 23:7-16
[2] Application of statistical process control in healthcare improvement: systematic review. Johan Thor, Jonas Lundberg, Jakob Ask, Jesper Olsson, Cheryl Carli, Karin Pukk Ha¨renstam, Mats Brommels. Qual Saf Health Care 2007;16:387–399. doi: 10.1136/qshc.2006.022194
[3] Operations Management, D.A. Collier, J.R. Evans(2007)
[4] Errors in patient specimen collection: application of statistical process control. Walter Sunny Dzik, Neil Beckman, Kathleen Selleng, Nancy Heddle, Zbigniew Szczepiorkowski, Silvano Wendel, and Michael Murphy for the Biomedical Excellence for Safer Transfusion (BEST) Collaborative (2008)
[5] Health Care Applications of Statistical Process Control: Examples Using the SASâ System Robert N. Rodriguez SAS Institute Inc. Cary, North Carolina, USA
Statistical Process Control is a methodology of statistical analysis used to discover special cause variation in a process. In healthcare, it is used to document that a critical process is in control and alert responsible parties should there be a deviation. A typical control chart is a graphical representation of the quality indicator, as either individual values or calculated subgroups with the data displayed sequentially and time ordered [Refer to illustration 1 in Appendix]. Horizontal lines represent the central tendency (mean), upper and lower control limits typically set at +3 standard deviations from the mean [1]. In this paper, we will list down the types of control charts available and guidelines to interpret it.
Types of Control Charts
In 1920s by Walter Shewhart developed it to improve industrial manufacturing. It first migrated to healthcare in laboratory settings and then into direct patient care applications [2].
There are four commonly used control charts [Refer to illustration 2, 3 in Appendix]. Control are categorized as upper (+) and lower (-).

A process is “in control” when it has the following characteristics [3]:
No points are outside the control limits – the traditional and most popular SPC chart guideline,
The number of points above and below the center line is about the same,
The points seem to fall randomly above and below the center line,
Most points, but not all, are near the centerline, and only a few are close to the control limits.
Evaluating the “patterns in the sample data” using guidelines such as [Refer to illustration 4 in Appendix]:
Eight points in a row above or below the center line
10 of 11 consecutive points above or below the center line
12 of 14 consecutive points above or below the center line
Two of three consecutive points in the outer one-third region between the center line and one of the control limits
Four of five consecutive points in the outer two-thirds region between the centerline and one of the control limits.
Basic Guidelines
In general, in applying statistical process control, we need to delineate the following:
The study and design objectives
Study settings - entire hospital, department etc
Fields of healthcare – anesthesia, pathology etc
Unit of analysis – Clinicians, patient, staff etc
Variables – Oxygen saturation, time to complete etc
Benefits – Impact assessment, quantify process variability etc
However, a number of special issues arise in health care applications of SPC. One of these is the question of what to measure. In health care applications, there is concern and debate about excessive emphasis on outcome metrics and report cards to the detriment of process understanding and improvement. Another issue is the problem of how to aggregate, adjust, and present rate data, used to make decisions [5].
Conclusion
Control charts provide an effective method to visualize data over a specific monitoring period while considering for boundary conditions. Usually the control limits are well within the specification limits for a capable process [Refer to illustration 5 in Appendix]. Continuing use of the control chart helps to check if the corrective action has resulted in an improved process. They allow hospital administrators to have a more engaging conversation with the physicians in the wake of the collected data. When shared between providers, control charts they drive higher standards of care. Patient identification and non-infectious hazards of transfusion are some typical bio-vigilance areas where software process control finds effective application.

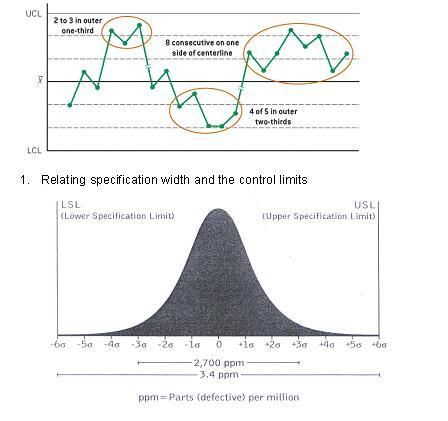
References
[1] Continuous quality improvement of perfusion practice. The role of electronic data collection and statistical control chart. RA Baker, RF Newland. Perfusion 2008 23:7-16
[2] Application of statistical process control in healthcare improvement: systematic review. Johan Thor, Jonas Lundberg, Jakob Ask, Jesper Olsson, Cheryl Carli, Karin Pukk Ha¨renstam, Mats Brommels. Qual Saf Health Care 2007;16:387–399. doi: 10.1136/qshc.2006.022194
[3] Operations Management, D.A. Collier, J.R. Evans(2007)
[4] Errors in patient specimen collection: application of statistical process control. Walter Sunny Dzik, Neil Beckman, Kathleen Selleng, Nancy Heddle, Zbigniew Szczepiorkowski, Silvano Wendel, and Michael Murphy for the Biomedical Excellence for Safer Transfusion (BEST) Collaborative (2008)
[5] Health Care Applications of Statistical Process Control: Examples Using the SASâ System Robert N. Rodriguez SAS Institute Inc. Cary, North Carolina, USA
Thursday, June 10, 2010
Process mapping in healthcare
A simple process map is depiction of sequence of information and material flow involving business entities (actors) using a standard set of symbols (BPMN/ADONIS) [1]. In 1921, Frank Gilberth introduced the first structured method for documenting process flows. Enhanced process mapping depicts functional units and roles using swim lanes. They start with level zero and progressively increase showing higher level of granularity. Although not exhaustive, the paper briefly describes the objectives, types, and best practices in process mapping.
Objectives of process maps
Process maps are fundamental to information capture. It is the building block of any new or improvement project.
Even though not always entire objective, a process map reproduces pre-existing reality. It allows us to contrast actual flow to the ideal flow.
They help getting past organizational silos [2].
We may employ process maps in a variety of scenarios like B2B (between organizations as in case of revenue cycle management), B2C (hospital patient interaction like outpatient and inpatient procedures), and B2E (employee to hospital interaction).
Discover complexity, redundancy, and blocks in the process, help to revaluate underlying assumption and predispositions
Identify location where there is a need to collect additional data and investigate [3].
Different types of process map
Process map comes in several flavors each highlight a different aspect and intended for a different audience.
High-level process flow shows core process within the organization. It shows the interaction between entities. Low-level process flow shows decision gates and loops
Cross-functional maps that use swim lanes, which allow the slotting of the activities among department or roles indicating the organizational structure and complexity involved.
Value stream maps that capture wait times, and additional attributes like inventory, throughput, and flow time.
SIPOC diagram which shows the high-level visual between suppliers, inputs, process, outcomes, and customers (refer to appendix).
There may be other variations of process maps, either tailored or derived to meet specific circumstances
Best Practices
Articulate the problem clearly and specifically using information available.
Involve the stakeholder group to participate in the modeling process
Determine the boundary or scope of the process to facilitate data collection and retain focus.
Determine and sequence the steps identifying the start and the end-points and the customer.
Start with high level and drill down progressively. Maintain consistency at each level.
Test for completeness of the map at each level.
The mapping exercise must be led by a facilitator who
Must have a neutral stand
Must set ground rules of engagement
Will create an environment for brain storming
Keep the exercise on track by parking contentious issues, keep focus on “value to the customer”
Conclusion
Process mapping spans across the “Define” and “Measure” phase of DMAIC framework of 6-Sigma and discovery of the “hidden plant” used in Lean. Define-Measure-Analyze-Improve-Control (DMAIC) is a framework for 6-Sigma implementation. The Define phase identifies the opportunity set for improvement and Measure phase quantifies the current state in terms of contextually relevant indicators. Hidden Plant is a lean construct denoting the unreported rework and scrap that goes into the outcome of a process.
Patient focused Integrated Care Pathways (ICP) is a good derivative of process map. They act templates to deliver care fostering evidence based medical practice. The ICP is not rigid but allows the variation in the clinical intervention depending on unique needs of the patient. The ICP serves as a reminder to document the variations in care from published guidelines. This in turn supports management of clinical risks and modification of the contents of the ICP.
Process mapping lays the foundation of any problem solving assignment. It also is an excellent tool to capture and transmit best practices in the organization and in the industry. Sophisticated information systems integrate process maps with packaged application making configuration and customization simpler and easy to maintain. Lean Six Sigma uses this methodology extensively to evaluate as-is state and create to-be state. It allows easy visualization of check- points to measure, monitor, and sustain activities in the process.
References
[1] eBusiness in Healthcare From eProcurement to Supply Chain Management Series: Health Informatics Hübner, Ursula; Elmhorst, Marc A. (Eds.)
[2] What’s in a care pathway? Towards a cultural cartography of the new NHS Ruth Pinder,Roland Petchey,Sara Shaw,Yvonne Carter. Sociology of Health & Illness Vol. 27 No. 6 2005 ISSN 0141–9889, pp. 759–779
[3] The Premier Healthcare Alliance. http://www.premierinc.com/about/mission/social-responsibility/cares/process-maps.pdf
[4] What is an integrated care pathway? Sue Middleton, Jane Barnett, David Reeves. Hayward Medical Communications. www.evidence-based-medicine.co.uk
[5] A toolkit for Redesign of healthcare. AHRQ. http://www.ahrq.gov/qual/toolkit/tkformf.htm
[6] http://facultyweb.berry.edu/jgrout/processmapping/Swim_Lane/swim_lane.html
[7] http://www.hfma.org/Templates/InteriorMaster.aspx?id=21198
Objectives of process maps
Process maps are fundamental to information capture. It is the building block of any new or improvement project.
Even though not always entire objective, a process map reproduces pre-existing reality. It allows us to contrast actual flow to the ideal flow.
They help getting past organizational silos [2].
We may employ process maps in a variety of scenarios like B2B (between organizations as in case of revenue cycle management), B2C (hospital patient interaction like outpatient and inpatient procedures), and B2E (employee to hospital interaction).
Discover complexity, redundancy, and blocks in the process, help to revaluate underlying assumption and predispositions
Identify location where there is a need to collect additional data and investigate [3].
Different types of process map
Process map comes in several flavors each highlight a different aspect and intended for a different audience.
High-level process flow shows core process within the organization. It shows the interaction between entities. Low-level process flow shows decision gates and loops
Cross-functional maps that use swim lanes, which allow the slotting of the activities among department or roles indicating the organizational structure and complexity involved.
Value stream maps that capture wait times, and additional attributes like inventory, throughput, and flow time.
SIPOC diagram which shows the high-level visual between suppliers, inputs, process, outcomes, and customers (refer to appendix).
There may be other variations of process maps, either tailored or derived to meet specific circumstances
Best Practices
Articulate the problem clearly and specifically using information available.
Involve the stakeholder group to participate in the modeling process
Determine the boundary or scope of the process to facilitate data collection and retain focus.
Determine and sequence the steps identifying the start and the end-points and the customer.
Start with high level and drill down progressively. Maintain consistency at each level.
Test for completeness of the map at each level.
The mapping exercise must be led by a facilitator who
Must have a neutral stand
Must set ground rules of engagement
Will create an environment for brain storming
Keep the exercise on track by parking contentious issues, keep focus on “value to the customer”
Conclusion
Process mapping spans across the “Define” and “Measure” phase of DMAIC framework of 6-Sigma and discovery of the “hidden plant” used in Lean. Define-Measure-Analyze-Improve-Control (DMAIC) is a framework for 6-Sigma implementation. The Define phase identifies the opportunity set for improvement and Measure phase quantifies the current state in terms of contextually relevant indicators. Hidden Plant is a lean construct denoting the unreported rework and scrap that goes into the outcome of a process.
Patient focused Integrated Care Pathways (ICP) is a good derivative of process map. They act templates to deliver care fostering evidence based medical practice. The ICP is not rigid but allows the variation in the clinical intervention depending on unique needs of the patient. The ICP serves as a reminder to document the variations in care from published guidelines. This in turn supports management of clinical risks and modification of the contents of the ICP.
Process mapping lays the foundation of any problem solving assignment. It also is an excellent tool to capture and transmit best practices in the organization and in the industry. Sophisticated information systems integrate process maps with packaged application making configuration and customization simpler and easy to maintain. Lean Six Sigma uses this methodology extensively to evaluate as-is state and create to-be state. It allows easy visualization of check- points to measure, monitor, and sustain activities in the process.
References
[1] eBusiness in Healthcare From eProcurement to Supply Chain Management Series: Health Informatics Hübner, Ursula; Elmhorst, Marc A. (Eds.)
[2] What’s in a care pathway? Towards a cultural cartography of the new NHS Ruth Pinder,Roland Petchey,Sara Shaw,Yvonne Carter. Sociology of Health & Illness Vol. 27 No. 6 2005 ISSN 0141–9889, pp. 759–779
[3] The Premier Healthcare Alliance. http://www.premierinc.com/about/mission/social-responsibility/cares/process-maps.pdf
[4] What is an integrated care pathway? Sue Middleton, Jane Barnett, David Reeves. Hayward Medical Communications. www.evidence-based-medicine.co.uk
[5] A toolkit for Redesign of healthcare. AHRQ. http://www.ahrq.gov/qual/toolkit/tkformf.htm
[6] http://facultyweb.berry.edu/jgrout/processmapping/Swim_Lane/swim_lane.html
[7] http://www.hfma.org/Templates/InteriorMaster.aspx?id=21198
Wednesday, June 2, 2010
History of healthcare quality
History of Healthcare Quality
The earliest notions of quality traces back to that of the “quality of life” elucidated in the Vedas. Subsequently, “quality of living” became the norm of a materialistically motivated society. Product and service quality are offshoots of this paradigm. However, in this brief paper we will focus on the history and evolution of quality in the recent past.
History of quality is probably as old as medical care itself.
Voluntary programs
Explicit and systematic use of death rates as a quality indicator by Florence Nightingale in mid 1800s marks the emergence of the quality assurance in healthcare.
The Flexner report in the early 1910[1] on the quality of medical education in the US was the first wake up call for reforming quality of medical education.
In 1915s, Ernest Codman gave the idea of outcome oriented medical audit which led to the establishment of the Hospital Standardization Program of the American College of Surgeons in 1918s[2].
Avedis Donabedian inspired by Codman conceived the Structure-Process-Outcome theory[3]. According to him, quality is a product of two factors. One is the science and technology of providing care and the second the application of first factor in practice. He proposed that the components of quality in healthcare consisted of efficacy, effectiveness, optimality, legitimacy, equity, and acceptability[4].
In 1950-60s, JCO adopted Donabedian’s theory and created quality assessment and improvement framework based on physical and staffing characteristics of caring for patients, the method of delivery, and the results of care. Over the years, JCO’s mission grew to embrace most healthcare settings[4].
Government regulatory programs
State licensing programs prevailed in 1800s.
In 1906, the FDA (Food and Drug Administration) undertook the national regulation of medication.
In 1935, the Social Security Act set the standards for maternal and child health.
In 1965 Medicare was institutionalized mandating principles central to hospital operations, staff credentialing, round the clock nursing care, and utilization review.
In 1980s, Healthcare Quality Improvement Initiative allowed professional standards review organizations to apply patient care algorithm to claims history and data set to screen cases and describe how well the care conforms to established guidelines[5].
On March 23, 2010, President Barack Obama signed The Patient Protection and Affordable Care Act into law. One week later, he signed The Health Care and Education Reconciliation Act of 2010, which made numerous changes to PPACA. This is likely to bring forth into play new patient care model, continuum of care, new AHRQ programs, metrics based reporting and a data driven national quality strategy.
Applying evidence to health delivery
Institute of Medicine defines quality in healthcare service as being safe, effective, patient centered, timely, efficient, and equitable[6]. There is a lag between discovery of efficacious forms of treatment and its incorporation into routine patient care[7]. In the recent past several private public partnerships like the Cochrane Collaboration and evidence based practice centers supported by AHRQ have emerged providing excellent models for quality care. Evidence based practice was started by Archie Cochrane in 1950s. It became apparent that it was not effective to train and encourage clinicians to independently find and apply best clinical practices. Quantitative systematic reviews began to appeal to the physician’s scientific outlook over qualitative “suggestions.” This eventually paved the way for healthcare to embrace the six sigma and lean frameworks.
Since 1980s there has been a steady transition from a needs based to an efficient profit making industry by adopting quality concepts like TQM, quality trilogy, and zero defects. Deming, Juran, and Crosby were the three quality gurus whose expansive work in the field of quality brought radical changes in other industries especially automotive. During 1980s, the John Hartford Foundation and Harvard Community Health Plan sponsor the national demonstration project on quality improvement in healthcare to determine if industrial TQM applies to healthcare[8].
Conclusion
We see that astute individuals, federal regulations, and other industrial best practices have shaped the quality in healthcare. Everyone understands the notions of superior quality. The challenge has been to have create mass momentum to make sure quality is not a matter of adherence but rather a thing of constant engagement.
References
[1] The Flexner Report at the Century Mark. A Wake-Up Call for Reforming Medical Education. Mike Mitka JAMA. 2010; 303(15):1465-1466
[2] Evaluation of the care of patients Codman Revisited. John D. Porterfield, M.D. Director, Joint Commission on Accreditation of Hospitals. Vol. 52, No. 1, January 1976
[3] The evolution of quality in the US health care industry: an old wine in a new bottle. Patrick Asubonteng, Karl J. McCleary and George Munchus University of Alabama, Birmingham, Alabama, USA
[4] An introduction to quality assurance in health care. Avedis Donabedian, Rashid Bashshur
[5] Luce JM, Bindman AB, Lee PR: A brief history of health care quality assessment and improvement in the United States. West J Med 1994; 160:263-268
[6] Crossing the Quality Chasm: A New Health System for the 21st Century (2001)
Institute of Medicine (IOM)
[7] Balas E, Boren S. Managing clinical knowledge for health care improvement. In: Bemmel J, McCray AT (eds). Section 1: health and clinical management. In Yearbook of Medical Informatics: Patient Centered Systems. Stuttgart, Germany: Schattauer Verlagsgesellschaft; 2000:65-70
[8] Quality in health care: theory, application, and evolution. Edition: 3 - 1995 Nancy O. Graham
The earliest notions of quality traces back to that of the “quality of life” elucidated in the Vedas. Subsequently, “quality of living” became the norm of a materialistically motivated society. Product and service quality are offshoots of this paradigm. However, in this brief paper we will focus on the history and evolution of quality in the recent past.
History of quality is probably as old as medical care itself.
Voluntary programs
Explicit and systematic use of death rates as a quality indicator by Florence Nightingale in mid 1800s marks the emergence of the quality assurance in healthcare.
The Flexner report in the early 1910[1] on the quality of medical education in the US was the first wake up call for reforming quality of medical education.
In 1915s, Ernest Codman gave the idea of outcome oriented medical audit which led to the establishment of the Hospital Standardization Program of the American College of Surgeons in 1918s[2].
Avedis Donabedian inspired by Codman conceived the Structure-Process-Outcome theory[3]. According to him, quality is a product of two factors. One is the science and technology of providing care and the second the application of first factor in practice. He proposed that the components of quality in healthcare consisted of efficacy, effectiveness, optimality, legitimacy, equity, and acceptability[4].
In 1950-60s, JCO adopted Donabedian’s theory and created quality assessment and improvement framework based on physical and staffing characteristics of caring for patients, the method of delivery, and the results of care. Over the years, JCO’s mission grew to embrace most healthcare settings[4].
Government regulatory programs
State licensing programs prevailed in 1800s.
In 1906, the FDA (Food and Drug Administration) undertook the national regulation of medication.
In 1935, the Social Security Act set the standards for maternal and child health.
In 1965 Medicare was institutionalized mandating principles central to hospital operations, staff credentialing, round the clock nursing care, and utilization review.
In 1980s, Healthcare Quality Improvement Initiative allowed professional standards review organizations to apply patient care algorithm to claims history and data set to screen cases and describe how well the care conforms to established guidelines[5].
On March 23, 2010, President Barack Obama signed The Patient Protection and Affordable Care Act into law. One week later, he signed The Health Care and Education Reconciliation Act of 2010, which made numerous changes to PPACA. This is likely to bring forth into play new patient care model, continuum of care, new AHRQ programs, metrics based reporting and a data driven national quality strategy.
Applying evidence to health delivery
Institute of Medicine defines quality in healthcare service as being safe, effective, patient centered, timely, efficient, and equitable[6]. There is a lag between discovery of efficacious forms of treatment and its incorporation into routine patient care[7]. In the recent past several private public partnerships like the Cochrane Collaboration and evidence based practice centers supported by AHRQ have emerged providing excellent models for quality care. Evidence based practice was started by Archie Cochrane in 1950s. It became apparent that it was not effective to train and encourage clinicians to independently find and apply best clinical practices. Quantitative systematic reviews began to appeal to the physician’s scientific outlook over qualitative “suggestions.” This eventually paved the way for healthcare to embrace the six sigma and lean frameworks.
Since 1980s there has been a steady transition from a needs based to an efficient profit making industry by adopting quality concepts like TQM, quality trilogy, and zero defects. Deming, Juran, and Crosby were the three quality gurus whose expansive work in the field of quality brought radical changes in other industries especially automotive. During 1980s, the John Hartford Foundation and Harvard Community Health Plan sponsor the national demonstration project on quality improvement in healthcare to determine if industrial TQM applies to healthcare[8].
Conclusion
We see that astute individuals, federal regulations, and other industrial best practices have shaped the quality in healthcare. Everyone understands the notions of superior quality. The challenge has been to have create mass momentum to make sure quality is not a matter of adherence but rather a thing of constant engagement.
References
[1] The Flexner Report at the Century Mark. A Wake-Up Call for Reforming Medical Education. Mike Mitka JAMA. 2010; 303(15):1465-1466
[2] Evaluation of the care of patients Codman Revisited. John D. Porterfield, M.D. Director, Joint Commission on Accreditation of Hospitals. Vol. 52, No. 1, January 1976
[3] The evolution of quality in the US health care industry: an old wine in a new bottle. Patrick Asubonteng, Karl J. McCleary and George Munchus University of Alabama, Birmingham, Alabama, USA
[4] An introduction to quality assurance in health care. Avedis Donabedian, Rashid Bashshur
[5] Luce JM, Bindman AB, Lee PR: A brief history of health care quality assessment and improvement in the United States. West J Med 1994; 160:263-268
[6] Crossing the Quality Chasm: A New Health System for the 21st Century (2001)
Institute of Medicine (IOM)
[7] Balas E, Boren S. Managing clinical knowledge for health care improvement. In: Bemmel J, McCray AT (eds). Section 1: health and clinical management. In Yearbook of Medical Informatics: Patient Centered Systems. Stuttgart, Germany: Schattauer Verlagsgesellschaft; 2000:65-70
[8] Quality in health care: theory, application, and evolution. Edition: 3 - 1995 Nancy O. Graham
Wednesday, May 26, 2010
Wednesday, April 21, 2010
A thing or two about change - William Bridges way - Final part
Launching the new beginning - facilitating people to emerge from the neutral zone and allow them to be fully expressed in the new order.
New starts are not enough. There could be several of them. A start is made on the formal date of announcement but people continue on the 2 train architecture. They have a shadow existence meeting their old team mates for lunch and going to their old bosses for advice. In such cases the new beginning has not been made because people have not put in their emotional commitment to do things the new way. The beginning is the final phase of the transition and the timing is not set by the bosses or the steering committees.
Sometimes when the neutral zone has been long enough, people resist beginnings for the following reasons:
1. Uncertainty about what this new future has in store for us
2. New beginnings may bring back the ghosts from the past
3. A new beginning creates the need to re-establish credibility and accountability
Beginnings may be facilitated by 4Ps
Purpose: Communicate why and how the new beginning was envisaged in terms of "what is in it for me". Sometimes there may be no purpose or the communication may be intentionally withheld leading to a loss of trust. Poor or mismanaged communication can seriously jeopardize any change program. The communication does not reflect the true intent of the leadership it means nothing to the people. This often leads to one start after another leaving people worn out without making any difference to the underlying scheme of things.
Picture: Imagery is very powerful. People need to create a mental picture of the new environment in which they will participate. This includes spatial layout, organization structure and experience. However a picture cannot replace the hard work of the leadership. Usually the change leaders typically go through their transition before they launch the change initiative. As a result they may fail to recognize the stages of transition the other are in. The imagery also has to be kept simple to allow people to relate to it meaningfully and not be overwhelmed.
Plan: Create a transition plan (different from a regular change plan). Transition plan is addresses at a personal level rather than a collective level. It is oriented to the process rather than the outcome.
Part to play: People need a part to may in the due course of the transition and in their relationship with others in the post change era. This allows people to gain firsthand knowledge on solving the problems associated with the change initiative and align themselves better.
As a final note, in order to reinforce the new beginning, there must be consistent, well aligned communication without sending conflicting messages. There must quick success navigating out the neutral zone with minimum time. The leadership must acknowledge the new identity. Symbolism is important as everything means something in the process of change.
New starts are not enough. There could be several of them. A start is made on the formal date of announcement but people continue on the 2 train architecture. They have a shadow existence meeting their old team mates for lunch and going to their old bosses for advice. In such cases the new beginning has not been made because people have not put in their emotional commitment to do things the new way. The beginning is the final phase of the transition and the timing is not set by the bosses or the steering committees.
Sometimes when the neutral zone has been long enough, people resist beginnings for the following reasons:
1. Uncertainty about what this new future has in store for us
2. New beginnings may bring back the ghosts from the past
3. A new beginning creates the need to re-establish credibility and accountability
Beginnings may be facilitated by 4Ps
Purpose: Communicate why and how the new beginning was envisaged in terms of "what is in it for me". Sometimes there may be no purpose or the communication may be intentionally withheld leading to a loss of trust. Poor or mismanaged communication can seriously jeopardize any change program. The communication does not reflect the true intent of the leadership it means nothing to the people. This often leads to one start after another leaving people worn out without making any difference to the underlying scheme of things.
Picture: Imagery is very powerful. People need to create a mental picture of the new environment in which they will participate. This includes spatial layout, organization structure and experience. However a picture cannot replace the hard work of the leadership. Usually the change leaders typically go through their transition before they launch the change initiative. As a result they may fail to recognize the stages of transition the other are in. The imagery also has to be kept simple to allow people to relate to it meaningfully and not be overwhelmed.
Plan: Create a transition plan (different from a regular change plan). Transition plan is addresses at a personal level rather than a collective level. It is oriented to the process rather than the outcome.
Part to play: People need a part to may in the due course of the transition and in their relationship with others in the post change era. This allows people to gain firsthand knowledge on solving the problems associated with the change initiative and align themselves better.
As a final note, in order to reinforce the new beginning, there must be consistent, well aligned communication without sending conflicting messages. There must quick success navigating out the neutral zone with minimum time. The leadership must acknowledge the new identity. Symbolism is important as everything means something in the process of change.
Wednesday, April 7, 2010
Nimble management
Introduction
Healthcare, like other sectors, has evolved to service a societal need. With a high number of players, interlocking systems and regulations, it is sensitive to the forces of people, process, and technology. The proposed reform will drive hospitals (also referred to as healthcare organization or provider in this essay) to be more competitive, bring down costs, and provide better outcomes. These are possible through transformational initiatives, none of which may be easy or intuitive. This essay highlights an alternate view of value and the factors that are crucial to succeed in instituting change.
Defining and locating value
Every organization exists because of a customer need it serves. A hospital helps a citizen to remain and stay healthy, and in the process creates and delivers value to the patient. Value may be defined as a product of quality of care, price paid for care and image of the hospital. Perception of value varies depending on type of care and other available choices e.g. patients seeking cardiac care may be fine spending high dollar amount as opposed to those seeking cure for common flu. Every interaction the patient has with the provider erodes or adds to patient loyalty. Value is greater than the sum of all services rendered to the patient. While it is convenient to work with an internal definition of value, a patient centric view is likely to fetch favorable results. A strong commitment to customer value increases organization’s competitive advantage, market share, and profitability. Drawing out a value stream is a key activity in the process of discovering this strategic measure of success.
Building blocks of a value stream
A value stream is a traditional six-sigma tool that allows us to analyze and align the sense of value within and beyond the enterprise. Admit-Discharge-Transfer-FollowUp (for in-patient) and Appointment-Diagnosis-Treatment-FollowUp (for outpatient) are typical value streams in health delivery. A business process is a set of activities that builds the value stream. An activity is a task or business function that has a hand-off either to another activity or to an end customer and has some measure of value. Activities may be of three types
• Those that create value
• Those that do not create value but cannot be dropped immediately
• Those that do not create value and are considered for elimination
While in the process of detailing the value stream, it is tempting to start reductionist, cost cutting changes mid way through the exercise. On the other hand, organizations need not go overboard with minutiae and must learn to prioritize the processes to balance the effort and gain. Surveys show that one of every five Medicare beneficiaries discharged from the hospital undergo readmission within 30 days, and half of non-surgical patients are readmitted to the hospital without having been seen by a doctor in an outpatient follow-up. There is opportunity in extending the scope of the value stream beyond the traditional enterprise boundaries. Providers, for example, can offer great value through post-discharge medication management. Creation of value stream forms a foundation for integrated health delivery. Such new models of business require innovative teams and leadership to succeed.
Team and Leadership
Most organizations are set up to operate in functional silos. During projects, resources from different departments combine to form a virtual team (matrix based). This is a winning formula so long as people are rational, share common motives and prioritize project goals in favor of departmental interests. However, in practice, managers struggle to get stakeholders aligned, provide contextual leadership, and retain a well performing team. One of the ways to have a focused team is to have it assigned to relevant business processes. The importance of team-based collaboration in healthcare is a difficult yet important agenda to pursue. Typically, the CxO owns the value stream and the dedicated senior management oversee each business process. Reformulation of the organization personnel along lines of business process often creates dramatic shifts in power. In general, people resist such initiatives making change management an important part of any innovation. The diagram below shows the connections between value stream, business process, activity, and organizational hierarchy.
A strategic transformation without strong leadership seldom has a chance to succeed. An empowered workforce that shares the strategic vision with its senior management creates an environment where change can thrive.
Socio technical aspect of change
Projects may fail for a number of reasons including lack of change management, resistance of stakeholders (including end user) and incorrect definition of value. Projects seldom fail for technical reasons as they do due to poor expectation and change management. Organizations need to recognize the interdependency between social and technical subsystems during periods of change. The technical subsystem consists of tools and techniques used to deliver favorable outcomes using given inputs. The social subsystem comprises of the people, knowledge, attitudes, needs, and chain of command affecting the workforce.
Psychological barriers
Altering knowledge and attitude is an effective and sustainable way to transform human behavior. Typical barriers in warming up to change include:
• Differences of opinion - people impacted by change often question its concept and are pessimistic about benefits arising from it
• Not participating in change - not acknowledging initiatives and not familiarizing with contents of the initiative
• Inertia of past practice has no motivation to adopt innovation
• Lack of preparation, lack of confidence and fear of job loss - during change, it is common for people to lose jobs. Paradoxically, it creates new jobs too. Employees who find it difficult keeping pace with change drop out and create skill gaps filled through lateral recruitment.
• External barriers – limited time, resource constraint, conflict between patient preferences and organization culture.
Illustrating the impact of barriers on change, a survey of over 800 participants at an annual electronic medical record (EMR) trade fair in the US in 2007 found that 19% of respondents reported that they had or were in the process of de-installing an EMR system.
Group dynamics
Diffusion of change across professions or groups depends on prevalent belief system and shared work experience. Lack of explicit tasks, lack of local leadership, and influence of professional socialization; all are factors that slow down change. Physicians train to be fiercely independent and exercise high levels of autonomy. Practice of medicine by its very nature is fluid with few formalized control mechanisms. Integrated inter-professional education is only starting to gain recognition in healthcare. Organizations realize collaboration and inter-professional relationship are critical success factors in patient care. Targeted workplace based training will prove to be vital for providers to manage group dynamics, keeping in mind that interventions aimed at one group could impact other professional groups.
The Brain factor
Any disruption in routine is potential change and is intimidating for most parts. Physiologically, the prefrontal cortex of the brain handles multiple threads of logic. However, its processing capacity is limited producing fatigue and possible anger upon reaching the threshold. Activity in the pre-frontal cortex burns a lot of metabolically expensive blood glucose. In contrast, the basal ganglia use blood sugar more economically and have higher processing capacity. This part of the brain stores the hardwired memories and habits and allows us to do the task mechanically. The interplay between the two parts of the brain gives us an insight into workforce resistance towards change. Traditional change management does not sufficiently address psychology and/or physiology. Reward-rebuke approach, unless applied system-wide, yields predictably low results. Surveys suggest that primary driver in workplace is neither money nor promotion, but a personal interest in the job, a conducive environment and fulfilling inter-professional relationship with colleagues.
When the prefrontal cortex perceives a well-meaning initiative as a threat, it soon becomes exhausted and just as quickly gets the individual to resist. One way to get past the brain defense is to help people to assimilate change contextually; get them to see the big picture and connect the dots. Brains scans show a tremendous amount of activity during moments of insights with the brain busy building complex connections. Good change management needs a lot of patience. Leaders have to resist their urge to be prescriptive. When the front line employees do not have the time window to make these connections on their own, they view change adversely. Addressing the physiological impulses constructively can be soothing to the prefrontal cortex.
Conclusion
“And let it be noted that there is no more delicate matter to take in hand, nor more dangerous to conduct, nor more doubtful in its success, than to set up as a leader in the introduction of changes. ” – Niccolo Machiavelli
Healthcare, like other sectors, has evolved to service a societal need. With a high number of players, interlocking systems and regulations, it is sensitive to the forces of people, process, and technology. The proposed reform will drive hospitals (also referred to as healthcare organization or provider in this essay) to be more competitive, bring down costs, and provide better outcomes. These are possible through transformational initiatives, none of which may be easy or intuitive. This essay highlights an alternate view of value and the factors that are crucial to succeed in instituting change.
Defining and locating value
Every organization exists because of a customer need it serves. A hospital helps a citizen to remain and stay healthy, and in the process creates and delivers value to the patient. Value may be defined as a product of quality of care, price paid for care and image of the hospital. Perception of value varies depending on type of care and other available choices e.g. patients seeking cardiac care may be fine spending high dollar amount as opposed to those seeking cure for common flu. Every interaction the patient has with the provider erodes or adds to patient loyalty. Value is greater than the sum of all services rendered to the patient. While it is convenient to work with an internal definition of value, a patient centric view is likely to fetch favorable results. A strong commitment to customer value increases organization’s competitive advantage, market share, and profitability. Drawing out a value stream is a key activity in the process of discovering this strategic measure of success.
Building blocks of a value stream
A value stream is a traditional six-sigma tool that allows us to analyze and align the sense of value within and beyond the enterprise. Admit-Discharge-Transfer-FollowUp (for in-patient) and Appointment-Diagnosis-Treatment-FollowUp (for outpatient) are typical value streams in health delivery. A business process is a set of activities that builds the value stream. An activity is a task or business function that has a hand-off either to another activity or to an end customer and has some measure of value. Activities may be of three types
• Those that create value
• Those that do not create value but cannot be dropped immediately
• Those that do not create value and are considered for elimination
While in the process of detailing the value stream, it is tempting to start reductionist, cost cutting changes mid way through the exercise. On the other hand, organizations need not go overboard with minutiae and must learn to prioritize the processes to balance the effort and gain. Surveys show that one of every five Medicare beneficiaries discharged from the hospital undergo readmission within 30 days, and half of non-surgical patients are readmitted to the hospital without having been seen by a doctor in an outpatient follow-up. There is opportunity in extending the scope of the value stream beyond the traditional enterprise boundaries. Providers, for example, can offer great value through post-discharge medication management. Creation of value stream forms a foundation for integrated health delivery. Such new models of business require innovative teams and leadership to succeed.
Team and Leadership
Most organizations are set up to operate in functional silos. During projects, resources from different departments combine to form a virtual team (matrix based). This is a winning formula so long as people are rational, share common motives and prioritize project goals in favor of departmental interests. However, in practice, managers struggle to get stakeholders aligned, provide contextual leadership, and retain a well performing team. One of the ways to have a focused team is to have it assigned to relevant business processes. The importance of team-based collaboration in healthcare is a difficult yet important agenda to pursue. Typically, the CxO owns the value stream and the dedicated senior management oversee each business process. Reformulation of the organization personnel along lines of business process often creates dramatic shifts in power. In general, people resist such initiatives making change management an important part of any innovation. The diagram below shows the connections between value stream, business process, activity, and organizational hierarchy.
A strategic transformation without strong leadership seldom has a chance to succeed. An empowered workforce that shares the strategic vision with its senior management creates an environment where change can thrive.
Socio technical aspect of change
Projects may fail for a number of reasons including lack of change management, resistance of stakeholders (including end user) and incorrect definition of value. Projects seldom fail for technical reasons as they do due to poor expectation and change management. Organizations need to recognize the interdependency between social and technical subsystems during periods of change. The technical subsystem consists of tools and techniques used to deliver favorable outcomes using given inputs. The social subsystem comprises of the people, knowledge, attitudes, needs, and chain of command affecting the workforce.
Psychological barriers
Altering knowledge and attitude is an effective and sustainable way to transform human behavior. Typical barriers in warming up to change include:
• Differences of opinion - people impacted by change often question its concept and are pessimistic about benefits arising from it
• Not participating in change - not acknowledging initiatives and not familiarizing with contents of the initiative
• Inertia of past practice has no motivation to adopt innovation
• Lack of preparation, lack of confidence and fear of job loss - during change, it is common for people to lose jobs. Paradoxically, it creates new jobs too. Employees who find it difficult keeping pace with change drop out and create skill gaps filled through lateral recruitment.
• External barriers – limited time, resource constraint, conflict between patient preferences and organization culture.
Illustrating the impact of barriers on change, a survey of over 800 participants at an annual electronic medical record (EMR) trade fair in the US in 2007 found that 19% of respondents reported that they had or were in the process of de-installing an EMR system.
Group dynamics
Diffusion of change across professions or groups depends on prevalent belief system and shared work experience. Lack of explicit tasks, lack of local leadership, and influence of professional socialization; all are factors that slow down change. Physicians train to be fiercely independent and exercise high levels of autonomy. Practice of medicine by its very nature is fluid with few formalized control mechanisms. Integrated inter-professional education is only starting to gain recognition in healthcare. Organizations realize collaboration and inter-professional relationship are critical success factors in patient care. Targeted workplace based training will prove to be vital for providers to manage group dynamics, keeping in mind that interventions aimed at one group could impact other professional groups.
The Brain factor
Any disruption in routine is potential change and is intimidating for most parts. Physiologically, the prefrontal cortex of the brain handles multiple threads of logic. However, its processing capacity is limited producing fatigue and possible anger upon reaching the threshold. Activity in the pre-frontal cortex burns a lot of metabolically expensive blood glucose. In contrast, the basal ganglia use blood sugar more economically and have higher processing capacity. This part of the brain stores the hardwired memories and habits and allows us to do the task mechanically. The interplay between the two parts of the brain gives us an insight into workforce resistance towards change. Traditional change management does not sufficiently address psychology and/or physiology. Reward-rebuke approach, unless applied system-wide, yields predictably low results. Surveys suggest that primary driver in workplace is neither money nor promotion, but a personal interest in the job, a conducive environment and fulfilling inter-professional relationship with colleagues.
When the prefrontal cortex perceives a well-meaning initiative as a threat, it soon becomes exhausted and just as quickly gets the individual to resist. One way to get past the brain defense is to help people to assimilate change contextually; get them to see the big picture and connect the dots. Brains scans show a tremendous amount of activity during moments of insights with the brain busy building complex connections. Good change management needs a lot of patience. Leaders have to resist their urge to be prescriptive. When the front line employees do not have the time window to make these connections on their own, they view change adversely. Addressing the physiological impulses constructively can be soothing to the prefrontal cortex.
Conclusion
“And let it be noted that there is no more delicate matter to take in hand, nor more dangerous to conduct, nor more doubtful in its success, than to set up as a leader in the introduction of changes. ” – Niccolo Machiavelli
Friday, March 19, 2010
A thing or two about change - William Bridges way - Part 2
Continuing on transitions
Often i hear programs started with lot of fanfare and then all of a sudden the environment is rife with rumors and disappointment. Characteristically marked by low motivation, low productivity and fatigue; people seem lost.
This is the neutral zone where people are in suspended animation trying to cope with life cut of from old ways of being and in anticipation of the new order. Well covered weaknesses are suddenly brought out into the open. A major concern in this state of affairs is that priorities get confused, risk of miscommunication. Under this polarized environment, it is easy for consensus to break apart and people say to themselves "get off the sinking ship Asap".
However, the neutral zone is also a time to plant seeds of innovation into the organizational psyche. It is a time weakness when organization culture is weak and offers minimal resistance to new ideas. In a well managed neutral zone, reorientation and redefinition may be effectively achieved. When people are ambivalent it is necessary and critical to address their doubts and reinforce the directional strategies.
When people pass through no-man land, they feel confident when they are able to remain interconnected. Training helps. Letting people know that we are all in it together helps them relate and bond better. The neutral zone is also a time to seek creative ideas inside the organization. Over the years in most companies the organizational immune system(the culture of business as usual) chokes off creativity. A neutral zone is a great platform to shake that feeling of status quo.
"When old words die out on the tongue, new melodies break forth from the heart; and where old tracks are lost, new country is revealed with its wonders"... Rabindranath Tagore
Often i hear programs started with lot of fanfare and then all of a sudden the environment is rife with rumors and disappointment. Characteristically marked by low motivation, low productivity and fatigue; people seem lost.
This is the neutral zone where people are in suspended animation trying to cope with life cut of from old ways of being and in anticipation of the new order. Well covered weaknesses are suddenly brought out into the open. A major concern in this state of affairs is that priorities get confused, risk of miscommunication. Under this polarized environment, it is easy for consensus to break apart and people say to themselves "get off the sinking ship Asap".
However, the neutral zone is also a time to plant seeds of innovation into the organizational psyche. It is a time weakness when organization culture is weak and offers minimal resistance to new ideas. In a well managed neutral zone, reorientation and redefinition may be effectively achieved. When people are ambivalent it is necessary and critical to address their doubts and reinforce the directional strategies.
When people pass through no-man land, they feel confident when they are able to remain interconnected. Training helps. Letting people know that we are all in it together helps them relate and bond better. The neutral zone is also a time to seek creative ideas inside the organization. Over the years in most companies the organizational immune system(the culture of business as usual) chokes off creativity. A neutral zone is a great platform to shake that feeling of status quo.
"When old words die out on the tongue, new melodies break forth from the heart; and where old tracks are lost, new country is revealed with its wonders"... Rabindranath Tagore
Tuesday, February 23, 2010
Challenges in EMR for physicians office
Reading bits and pieces of information from the internet and different viewpoints, it is quite evident that HIT implementation in a acute care hospital is not the same as implementing EMR for a physician's office.
Interestingly there are around 400 vendors( about 70 certified ones) for EMR. The average de-installation rate is close to 20%
While it is important for an EMR vendor to have a strong customer base and financial resources to keep updating features, it is important that they have the consulting skills and be able to help their clients derive business value from their IT investment. However smaller vendors have attractive pricing policy to compensate for lack of competencies.
EPIC systems for example is a product developed by the vendor internally and not put together through an acquisition plan. This gives them an advantage in terms of application lineage. It allows them to create lite version of the product to cater to a better range of customer needs.
According to Fox Group, 8 critical functions for a physicians office are
- Physician Inbasket
- Medcial Assistance Inbasket
- Patient scheduling
- Patient Check In
- Encounter documentation including workflows. CPT and DRG coding support
- Patient Check Out
- BIlling and Collections
- Patient Portal, reports etc
Moving from paper to computer is an important transition. Meaningful use increases in functionality and sophistication over period of time. Shift in incentives includes incentives payments, possible government financing. In order to have a operationally efficient EMR system and a "meaningful" the following are good steps to follow
- Observe a due diligence
- Assess operation consequences including changes in workflow
- Have a implementation plan and a team to carry it out
- Anticipate and handle disruption during implementation and conversion
- Balance between features. Dont overpurchase or be limited
- Get it right the first time is critical.
Interestingly there are around 400 vendors( about 70 certified ones) for EMR. The average de-installation rate is close to 20%
While it is important for an EMR vendor to have a strong customer base and financial resources to keep updating features, it is important that they have the consulting skills and be able to help their clients derive business value from their IT investment. However smaller vendors have attractive pricing policy to compensate for lack of competencies.
EPIC systems for example is a product developed by the vendor internally and not put together through an acquisition plan. This gives them an advantage in terms of application lineage. It allows them to create lite version of the product to cater to a better range of customer needs.
According to Fox Group, 8 critical functions for a physicians office are
- Physician Inbasket
- Medcial Assistance Inbasket
- Patient scheduling
- Patient Check In
- Encounter documentation including workflows. CPT and DRG coding support
- Patient Check Out
- BIlling and Collections
- Patient Portal, reports etc
Moving from paper to computer is an important transition. Meaningful use increases in functionality and sophistication over period of time. Shift in incentives includes incentives payments, possible government financing. In order to have a operationally efficient EMR system and a "meaningful" the following are good steps to follow
- Observe a due diligence
- Assess operation consequences including changes in workflow
- Have a implementation plan and a team to carry it out
- Anticipate and handle disruption during implementation and conversion
- Balance between features. Dont overpurchase or be limited
- Get it right the first time is critical.
Saturday, February 20, 2010
A thing or two about change - William Bridges way - Part 1
I was reading Managing Transitions by William Bridges. A great read for anyone into IT consulting.
There is a distinction between change and transition. Change is situational characterized by the movement from one state to the other. It is outcome driven. Transition is psychological, a journey that makes change possible. It is the process by which people internalize and come to terms with the new order introduced by change. Most often than not, an apparently logical and well intended change fails miserably because the tansition is mismanaged.
The first step of transition is to recognize that it is time to bring the curtain down on the old ways; at least some of them. So transition starts with an ending of sorts. It is critical for change managers and project managers to understand the while people have no inhibition to the very outcome generated by the change, they naturally tend to resist the losses and endings that come with it.
Often the change creates a series of Brownian collisions making a far reaching impact. Everyone is losing something and many of the losses are not concrete because change is perceived through the filters of the mind.
Dynamic leadership
Enables the workforce to accept the realities of change
Does not get upset with overreaction
Acknowledge the losses openly and tries to compensate for it(does not have to be monetarily)
The underlying substratum of change is communication. It important that people are not misinformed (usually misinformation spreads at the speed of light). It pays to reiterate what's coming to an end and what is new order in Simple messages. Not all things about the past is necessarily bad and so it deserves some reverance. But it is important to show how the past has ceded the way to the future to unfold like the pupa has to give itself up to become the butterfly.
There is a distinction between change and transition. Change is situational characterized by the movement from one state to the other. It is outcome driven. Transition is psychological, a journey that makes change possible. It is the process by which people internalize and come to terms with the new order introduced by change. Most often than not, an apparently logical and well intended change fails miserably because the tansition is mismanaged.
The first step of transition is to recognize that it is time to bring the curtain down on the old ways; at least some of them. So transition starts with an ending of sorts. It is critical for change managers and project managers to understand the while people have no inhibition to the very outcome generated by the change, they naturally tend to resist the losses and endings that come with it.
Often the change creates a series of Brownian collisions making a far reaching impact. Everyone is losing something and many of the losses are not concrete because change is perceived through the filters of the mind.
Dynamic leadership
Enables the workforce to accept the realities of change
Does not get upset with overreaction
Acknowledge the losses openly and tries to compensate for it(does not have to be monetarily)
The underlying substratum of change is communication. It important that people are not misinformed (usually misinformation spreads at the speed of light). It pays to reiterate what's coming to an end and what is new order in Simple messages. Not all things about the past is necessarily bad and so it deserves some reverance. But it is important to show how the past has ceded the way to the future to unfold like the pupa has to give itself up to become the butterfly.
Wednesday, February 10, 2010
Knowledge Workers
I am sure much has been talked about knowledge workers. Today i had a chance to listen to a video presentation (dated by a few good years) from a professor in Stanford. It appears that quite a bit of it is still real and valid today.I thought it might be worthwhile to put some of those here.
Organization architectures goes beyond the traditional org. structures (from the value chain of Mr. Porter) to include the IT infrastructure and the physical design of the workplace. Interesting example - Office building in Sun Microsystems at Menlow Park is superwide. The rationale is that Sun wants its people to work in teams and they want the teams to be able to walk the stairs together. A subtle effort to speed up communication.
The traditional parent-child (mentor-mentee) relationship has been replaced by peer-to-peer relationship creating flat organizations. The condition of employee retention hinges on the ability of the individual to being value to the table. Increasingly, authoritative heirarchy is being replaced by accountability style of management. Career advancement that was once seen as vertical progress is now more about moving sideways, being current and innovative. Hiring that once based on efficiency has now moved to effectivity. A cultural fit is more important than a skill fit. This becomes vital with more temporary and contract workers. With organizations experimenting new models, the role of people in hub positions has become markedly critical. These are project managers, consultants who act as synaptic nodes between a variety of stakeholders, wearing different hats. They influence without much authority and create more intangible deliverables.
A few themes for our observation.
Let us move away from uniformity and celebrate diveristy by glueing it together with culture and values. Different people work with different management styles. For some constructive confrontation works and for some other consensus and collaboration is the way to go.
The intensity of the knowledge worker has been mentally working round the clock resulting in a a quicker burnout. People need a escape hatch to recharge themselves.
A high employee churn is not necessarily a negative indicator. Leveraging ex- employee alumni is like creating a brand equity in the lateral workforce market.
In a hub style environment, boundary setting is an abosolute must to facilitate quick decision making and conflict resolution. The C-level needs to be well connected with the ground troops to convert resource and competencies into compettitive advantage.
Getting to know the kinetics of this thought process helps me appreciate the organization transition.
Organization architectures goes beyond the traditional org. structures (from the value chain of Mr. Porter) to include the IT infrastructure and the physical design of the workplace. Interesting example - Office building in Sun Microsystems at Menlow Park is superwide. The rationale is that Sun wants its people to work in teams and they want the teams to be able to walk the stairs together. A subtle effort to speed up communication.
The traditional parent-child (mentor-mentee) relationship has been replaced by peer-to-peer relationship creating flat organizations. The condition of employee retention hinges on the ability of the individual to being value to the table. Increasingly, authoritative heirarchy is being replaced by accountability style of management. Career advancement that was once seen as vertical progress is now more about moving sideways, being current and innovative. Hiring that once based on efficiency has now moved to effectivity. A cultural fit is more important than a skill fit. This becomes vital with more temporary and contract workers. With organizations experimenting new models, the role of people in hub positions has become markedly critical. These are project managers, consultants who act as synaptic nodes between a variety of stakeholders, wearing different hats. They influence without much authority and create more intangible deliverables.
A few themes for our observation.
Let us move away from uniformity and celebrate diveristy by glueing it together with culture and values. Different people work with different management styles. For some constructive confrontation works and for some other consensus and collaboration is the way to go.
The intensity of the knowledge worker has been mentally working round the clock resulting in a a quicker burnout. People need a escape hatch to recharge themselves.
A high employee churn is not necessarily a negative indicator. Leveraging ex- employee alumni is like creating a brand equity in the lateral workforce market.
In a hub style environment, boundary setting is an abosolute must to facilitate quick decision making and conflict resolution. The C-level needs to be well connected with the ground troops to convert resource and competencies into compettitive advantage.
Getting to know the kinetics of this thought process helps me appreciate the organization transition.
Monday, February 8, 2010
Revenue Cycle Management in Healthcare organization
Revenue cycle management is one of the most complex operations in the healthcare settings. Below is a diagram to illustrate the same. My thanks to my friend and classmate Clay Demler for giving me a flow chart.


Tuesday, February 2, 2010
Information standards in healthcare Part 2 (final)
Writing anything on information standards without the mention of HL7 will be quite meaningless.
HL7 (Health Level Seven) is a Standards Developing Organization accredited by ANSI. It has complied a collection of message formats and related clinical standards that loosely represents clinical information.
Key observation:
HL7 was initiated to speeden up data interface and exchange between computer application and systems within or connected to one healthcare enterprise; irrespective of architecture, programming language or platform. It is less far reaching that HIPAA which is targetted at transforming business and patient are processes.
HL7 is similar to EDI but developed ground up. HIPAA is derived from X12 standards.
Under HIPAA the addtional information to support a patient claim or encoutner must be in HL7 format. THe likely transaction used in HIPAA are 275, 277, 278, 835.
Refer to Corepoint health for more information.
THe most commonly used message types are
ACK – General acknowledgement
ADT – Admit discharge transfer
BAR – Add/change billing account
DFT – Detailed financial transaction
MDM – Medical document management
MFN – Master files notification
ORM – Order (Pharmacy/treatment)
ORU – Observation result (Unsolicited)
QRY – Query, original mode
RAS – Pharmacy/treatment administration
RDE – Pharmacy/treatment encoded order
RGV – Pharmacy/treatment give
SIU – Scheduling information unsolicited
Some videos on HL7 worth listening to:
HL7 & Healthcare Interfacing Videos | Corepoint Health
Posted using ShareThis
HL7 (Health Level Seven) is a Standards Developing Organization accredited by ANSI. It has complied a collection of message formats and related clinical standards that loosely represents clinical information.
Key observation:
HL7 was initiated to speeden up data interface and exchange between computer application and systems within or connected to one healthcare enterprise; irrespective of architecture, programming language or platform. It is less far reaching that HIPAA which is targetted at transforming business and patient are processes.
HL7 is similar to EDI but developed ground up. HIPAA is derived from X12 standards.
Under HIPAA the addtional information to support a patient claim or encoutner must be in HL7 format. THe likely transaction used in HIPAA are 275, 277, 278, 835.
Refer to Corepoint health for more information.
THe most commonly used message types are
ACK – General acknowledgement
ADT – Admit discharge transfer
BAR – Add/change billing account
DFT – Detailed financial transaction
MDM – Medical document management
MFN – Master files notification
ORM – Order (Pharmacy/treatment)
ORU – Observation result (Unsolicited)
QRY – Query, original mode
RAS – Pharmacy/treatment administration
RDE – Pharmacy/treatment encoded order
RGV – Pharmacy/treatment give
SIU – Scheduling information unsolicited
Some videos on HL7 worth listening to:
HL7 & Healthcare Interfacing Videos | Corepoint Health
Posted using ShareThis
Tuesday, January 26, 2010
Information standards in healthcare Part 1
The healthcare world has a headspinning proportion of standards relevant to information management. Getting useful information on internet about such things is easier said than done. My thanks to all those who had some genuine information out there for the reentrants like me.
Title II, Administrative Simplification of the HIPAA of 1996 called for efficient and electronic transaction for administration and finance in healthcare. It impacted all "covered entities". American National Standards Institute (ANSI)standard was preferred by the federal regulators. Some of the key ANSI standards are Accredited Standards Committee(ASC) X12, National Council for Prescription Drug Program (NCPDP), Health Level Seven (HL7). An episode of health care may involve several HL7 messages and X12 transactions running sequentially or concurrently, all communicating about the the same health care “objects” or events. This may raise the issues of interoperability id data semantics to not match.
New version of current transactions and new transacation are being worked upon.The currently used formats being upgraded from X12 Version 4010A1 to 5010 and from NCPDP 5.1to D.0 (Refer to http://www.cms.hhs.gov/Versions5010andD0/downloads/5010_Provider_Natl_Conf_Call_06092009.pdf for more information). Jan 1, 2012 is the cutoff for all old transaction.
An over view of the interaction of X12 messages and HIPAA cross reference is given below:
HIPAA Transaction X12.
Claim 837
Eligibility 270/271
Auth. Request 278
Claim Status 276/277
Enrollment 834
Remittance 835
Premium Pmt. 820
Attachment 275
ACK TA1/997


Note: The UB04, CMS 1500 are standards to align the paper form to the electronic format.The CMS-1500 is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of claims.
In terms of the the contents of the electronic message, some other terms are relevant.
Diagnosis Related Group (DRG) is essentially categories under which reimbursements are sought for diseases classified under International Classification of Diseases (ICD-9). ICD-9 is used for inpatient and outpatient diagnosis and inpatient procedures (ICD-9-CM). Current Procedure Terminology (CPT) is used for outpatient services rendered.
Title II, Administrative Simplification of the HIPAA of 1996 called for efficient and electronic transaction for administration and finance in healthcare. It impacted all "covered entities". American National Standards Institute (ANSI)standard was preferred by the federal regulators. Some of the key ANSI standards are Accredited Standards Committee(ASC) X12, National Council for Prescription Drug Program (NCPDP), Health Level Seven (HL7). An episode of health care may involve several HL7 messages and X12 transactions running sequentially or concurrently, all communicating about the the same health care “objects” or events. This may raise the issues of interoperability id data semantics to not match.
New version of current transactions and new transacation are being worked upon.The currently used formats being upgraded from X12 Version 4010A1 to 5010 and from NCPDP 5.1to D.0 (Refer to http://www.cms.hhs.gov/Versions5010andD0/downloads/5010_Provider_Natl_Conf_Call_06092009.pdf for more information). Jan 1, 2012 is the cutoff for all old transaction.
An over view of the interaction of X12 messages and HIPAA cross reference is given below:
HIPAA Transaction X12.
Claim 837
Eligibility 270/271
Auth. Request 278
Claim Status 276/277
Enrollment 834
Remittance 835
Premium Pmt. 820
Attachment 275
ACK TA1/997

Note: The UB04, CMS 1500 are standards to align the paper form to the electronic format.The CMS-1500 is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of claims.
In terms of the the contents of the electronic message, some other terms are relevant.
Diagnosis Related Group (DRG) is essentially categories under which reimbursements are sought for diseases classified under International Classification of Diseases (ICD-9). ICD-9 is used for inpatient and outpatient diagnosis and inpatient procedures (ICD-9-CM). Current Procedure Terminology (CPT) is used for outpatient services rendered.
Tuesday, January 19, 2010
EMR - Where are we and what's in it
The Health Information Technology for Economic and Clinical Health Act has pushed the EMR agenda into reality. An interesting handshake between Walmart, eCW and Dell is worth noting (http://www.nytimes.com/2009/03/11/business/11record.html?_r=4&hp).
Walmart plans to team its Sam’s Club division with Dell for computers and eClinicalWorks. Wal-Mart says its package deal of hardware, software, installation, maintenance and training will make the technology more accessible and affordable, undercutting rival health information technology suppliers by as much as half.The Sam’s Club offering, to be made available this spring, will be under $25,000 for the first physician in a practice, and about $10,000 for each additional doctor. After the installation and training, continuing annual costs for maintenance and support will be $4,000 to $6,500 a year, the company estimates. Wal-Mart says it had explored the opportunity in health information technology long before the presidential election. About 200,000 health care providers, mostly doctors, are among Sam Club’s 47 million members.The company’s test bed for the technology it will soon offer physicians has been its own health care clinics, staffed by third-party physicians and nurses. Started in September 2006, 30 such clinics are now in stores in eight states. The clinics use the technology Wal-Mart will offer to physicians
How ready is the heatlhcare sector in terms of EMR adoption: A quick preview from HIMSSanalytics.org (The State of U.S. Hospitals Relative to Achieving Meaningful Use Measurements By Michael W. Davis Executive Vice President – HIMSS Analytics)

Walmart plans to team its Sam’s Club division with Dell for computers and eClinicalWorks. Wal-Mart says its package deal of hardware, software, installation, maintenance and training will make the technology more accessible and affordable, undercutting rival health information technology suppliers by as much as half.The Sam’s Club offering, to be made available this spring, will be under $25,000 for the first physician in a practice, and about $10,000 for each additional doctor. After the installation and training, continuing annual costs for maintenance and support will be $4,000 to $6,500 a year, the company estimates. Wal-Mart says it had explored the opportunity in health information technology long before the presidential election. About 200,000 health care providers, mostly doctors, are among Sam Club’s 47 million members.The company’s test bed for the technology it will soon offer physicians has been its own health care clinics, staffed by third-party physicians and nurses. Started in September 2006, 30 such clinics are now in stores in eight states. The clinics use the technology Wal-Mart will offer to physicians
How ready is the heatlhcare sector in terms of EMR adoption: A quick preview from HIMSSanalytics.org (The State of U.S. Hospitals Relative to Achieving Meaningful Use Measurements By Michael W. Davis Executive Vice President – HIMSS Analytics)

Short Primer on HIT data
As i trudge along unlearning and relearning fundamentals in my class, i thought it might be a good idea to pen down some of it.
Some key terminologies
Data: Empirical observations, symbols, numbers. They simply exist with no structure. A "know nothing" stage
Information: Data organized with relationships. No necessarily useful but is the building block for eveything else.. A "know what" stage
Knowledge: Information that has a pattern and is useful. Enables decision making. A "know how" stage
Understanding: Allows use of the known based on principles and fosters new knowledge. A "know why" stage
The types of information in a typical healthcare setting are as follows:
Internal , External and Comparative
Internal information may relate to
Patient encounter (patient-specific or aggregate) & (clinical or administrative)
General Operations
Exernal information is knowledge based
Comparative information - Outcome measure (over a period of time or against standard)
Common categories of benchmarking are patient satisfaction, practice patterns, health plans, clinical indicators, population measures.
A few key standards to note
ICD-9-CM is also known as international classification of disease Clinical modification. It is used to determine diagnostic related group. Critical to accurate institutional reimbursement
CPT - Current procedural terminology. It is used to provide information on medical and surgical services.
CMS 1450 and CMS 1500 are 2 common billing standards
A health executive needs to be sure of the source of the information, its accuracy and semantics. Given multiple standards agencies and multiple forces acting upon the healthcare organization, it is important to have a common understanding of the terms. A good reference is the document embedded below. It is taken as from the hhs.gov website as a reference.
Some key takeaways from a definition standpoint are given below:
EMR - Electronic medical record - Maintain within organization boundaries and owned by the provider
EHR - Interoperable data maintained to be shared across organizations in conformance with national standards
PHR - Personal heatlh record - Individually owned and maintained
Health Information Exchange is the entity that will facilitate the EHR exchange nationally. They will work with Regional Extension Centers (Health Information Organization). HIOs will collaborate with Regional Health Information Organization which are collaborated network between providers in a specific geography.
Some key terminologies
Data: Empirical observations, symbols, numbers. They simply exist with no structure. A "know nothing" stage
Information: Data organized with relationships. No necessarily useful but is the building block for eveything else.. A "know what" stage
Knowledge: Information that has a pattern and is useful. Enables decision making. A "know how" stage
Understanding: Allows use of the known based on principles and fosters new knowledge. A "know why" stage
The types of information in a typical healthcare setting are as follows:
Internal , External and Comparative
Internal information may relate to
Patient encounter (patient-specific or aggregate) & (clinical or administrative)
General Operations
Exernal information is knowledge based
Comparative information - Outcome measure (over a period of time or against standard)
Common categories of benchmarking are patient satisfaction, practice patterns, health plans, clinical indicators, population measures.
A few key standards to note
ICD-9-CM is also known as international classification of disease Clinical modification. It is used to determine diagnostic related group. Critical to accurate institutional reimbursement
CPT - Current procedural terminology. It is used to provide information on medical and surgical services.
CMS 1450 and CMS 1500 are 2 common billing standards
A health executive needs to be sure of the source of the information, its accuracy and semantics. Given multiple standards agencies and multiple forces acting upon the healthcare organization, it is important to have a common understanding of the terms. A good reference is the document embedded below. It is taken as from the hhs.gov website as a reference.
Some key takeaways from a definition standpoint are given below:
EMR - Electronic medical record - Maintain within organization boundaries and owned by the provider
EHR - Interoperable data maintained to be shared across organizations in conformance with national standards
PHR - Personal heatlh record - Individually owned and maintained
Health Information Exchange is the entity that will facilitate the EHR exchange nationally. They will work with Regional Extension Centers (Health Information Organization). HIOs will collaborate with Regional Health Information Organization which are collaborated network between providers in a specific geography.
Wednesday, January 6, 2010
My Takeaway from Michael L George’s Lean Six Sigma for Services Final Part
The nature of service work makes it difficult to find out what needs change and how to transform. The work product is often invisible making it difficult to track the flow. Service industry is has a long tradition of being individualistic. People are protective about losing their creativity to standardization. It is vital to engage the people instead of enforcing compliance. Data in service industry is neither organized nor readily available. More often than not decisions are judgment or Delphi based. People do not respond to inputs/instructions as do machines. The sheer unpredictability of human behavior is daunting.
Recognizing waste in service is critical to a successful LSS initiative:
• Over processing – PMI calls it “Gold Plating.” It may also include inefficient iterations of work product, unnecessary handoffs, creation of cumbersome documentation, etc.
• Transportation and motion – A lot of effort goes in information chasing. The data or the person having the data is difficult to reach out. The lack of resources may be result in information waiting at desktops for being processed.
• Inventory and waiting time – Non-value added work upstream increases downstream wait time. Skill and resource bottlenecks are also contributors
• Defect – Lost communication, miscommunication result in work product being incomplete or contrary to customer needs.
• Overproduction – Poor prioritization or work qualification leads to over commit and under deliver
Some useful ideas for running initiatives in service industry:
• Be creative in meetings – Use the meeting times wisely. Collect data offline. Use meetings to analyze information, make decisions, and have concrete takeaways.
• Look for obvious quick hit opportunities – Pick up low hanging fruit and use the results of those initiatives to promote initiatives in more critical areas.
• Use improvement events like Kaizen (traditional or improvised) to generate energy and immediate gains.
• Reach out beyond team boundaries.
• Set realistic expectation – A single projects does not produce best in class improvements. Processes are generally littered with variation and not managed with even a general understanding of velocity and flow. These are 2 distinct deficiencies and need to addressed separately
• Pay attention to team composition – Dr. Belbin’s model offers a good guideline, manage expectation
• Be conscious of your audience – Improvise tools and method to suit the organization, lead by example.
DMAIC
A typical LSS project begins with a one-page charter with sufficient data to compute benefits, resource requirements, and ROIC estimates. Basic elements of DEFINE include
• Consensus on the problem
• Understand the project link to corporate strategy and ROIC
• Agree on project boundaries/scope of value stream
• Know the key metrics or indicators of success (people must be able to make sense of it)
MEASURE bases on data and separates Six Sigma from a general process tinkering activity. Common data gathering challenges include too little data, no data, too much data, and irrelevant data. Useful steps in measure are
• Establish baseline – Measure useful data like things-in-process, average completion rate, cycle time, first pass yield, approvals/handoffs, downtime/learning curve, defects that affect the customer, and complexity
• Impartially observe the process – Watch people, track emails, phone calls, set goals for observation, ensure consistent data collection
The purpose of ANALYZE is to make sense of the data collected so far. The key part is to stick to the data and not be colored by individual experience and opinions. It may use scatter diagram to correlate variables. Time trap analysis can identify improvement areas.
IMPROVE applies standard tools implement brainstormed alternatives. The tools include those for setup time reduction (learning curve, upstream batching), 5S (De-cluttering), and queuing methods for decongestion (Staff pooling/cross training, task slotting/triaging, back up capacity, variation reduction). In a philosophical sense, nothing really changes except that the universe rearranges to be more efficient. Things like sponsor support and communication are of essence in this stage
A standard rule says we must spend time on a task only 10 times as much as it takes to set the task up. Some important questions for setup time reduction.
• What is delaying the start of work
• What factors lead to work interruption
• What inhibits moving at full throttle
• Is there any redundancy
• Is there a possibility for rationalization/ task offloading/ streamlining
• How to apply statistical control
The aim of CONTROL is to preserve the gains made in improve till yet another generation of improvement happens. Key steps are
• Documentation – to ensure people don’t slip back into old habits
• Convert results into currency – Project need financial validation and verification not be mere feel good factor. Not all gains are financially tangible. Verify the results at later points in time to ensure consistent returns
• Set up alerting mechanism to catch when the process spins out of control
Control is the cross over point when the process owner will take charge.
The book is an amazing read.
Recognizing waste in service is critical to a successful LSS initiative:
• Over processing – PMI calls it “Gold Plating.” It may also include inefficient iterations of work product, unnecessary handoffs, creation of cumbersome documentation, etc.
• Transportation and motion – A lot of effort goes in information chasing. The data or the person having the data is difficult to reach out. The lack of resources may be result in information waiting at desktops for being processed.
• Inventory and waiting time – Non-value added work upstream increases downstream wait time. Skill and resource bottlenecks are also contributors
• Defect – Lost communication, miscommunication result in work product being incomplete or contrary to customer needs.
• Overproduction – Poor prioritization or work qualification leads to over commit and under deliver
Some useful ideas for running initiatives in service industry:
• Be creative in meetings – Use the meeting times wisely. Collect data offline. Use meetings to analyze information, make decisions, and have concrete takeaways.
• Look for obvious quick hit opportunities – Pick up low hanging fruit and use the results of those initiatives to promote initiatives in more critical areas.
• Use improvement events like Kaizen (traditional or improvised) to generate energy and immediate gains.
• Reach out beyond team boundaries.
• Set realistic expectation – A single projects does not produce best in class improvements. Processes are generally littered with variation and not managed with even a general understanding of velocity and flow. These are 2 distinct deficiencies and need to addressed separately
• Pay attention to team composition – Dr. Belbin’s model offers a good guideline, manage expectation
• Be conscious of your audience – Improvise tools and method to suit the organization, lead by example.
DMAIC
A typical LSS project begins with a one-page charter with sufficient data to compute benefits, resource requirements, and ROIC estimates. Basic elements of DEFINE include
• Consensus on the problem
• Understand the project link to corporate strategy and ROIC
• Agree on project boundaries/scope of value stream
• Know the key metrics or indicators of success (people must be able to make sense of it)
MEASURE bases on data and separates Six Sigma from a general process tinkering activity. Common data gathering challenges include too little data, no data, too much data, and irrelevant data. Useful steps in measure are
• Establish baseline – Measure useful data like things-in-process, average completion rate, cycle time, first pass yield, approvals/handoffs, downtime/learning curve, defects that affect the customer, and complexity
• Impartially observe the process – Watch people, track emails, phone calls, set goals for observation, ensure consistent data collection
The purpose of ANALYZE is to make sense of the data collected so far. The key part is to stick to the data and not be colored by individual experience and opinions. It may use scatter diagram to correlate variables. Time trap analysis can identify improvement areas.
IMPROVE applies standard tools implement brainstormed alternatives. The tools include those for setup time reduction (learning curve, upstream batching), 5S (De-cluttering), and queuing methods for decongestion (Staff pooling/cross training, task slotting/triaging, back up capacity, variation reduction). In a philosophical sense, nothing really changes except that the universe rearranges to be more efficient. Things like sponsor support and communication are of essence in this stage
A standard rule says we must spend time on a task only 10 times as much as it takes to set the task up. Some important questions for setup time reduction.
• What is delaying the start of work
• What factors lead to work interruption
• What inhibits moving at full throttle
• Is there any redundancy
• Is there a possibility for rationalization/ task offloading/ streamlining
• How to apply statistical control
The aim of CONTROL is to preserve the gains made in improve till yet another generation of improvement happens. Key steps are
• Documentation – to ensure people don’t slip back into old habits
• Convert results into currency – Project need financial validation and verification not be mere feel good factor. Not all gains are financially tangible. Verify the results at later points in time to ensure consistent returns
• Set up alerting mechanism to catch when the process spins out of control
Control is the cross over point when the process owner will take charge.
The book is an amazing read.
Subscribe to:
Posts (Atom)